HBF is pleased to connect our blog readers to Christine Kukka’s monthly HBV Journal Review that she writes for the HBV Advocate. The journal presents the latest in hepatitis B research, treatment, and prevention from recent academic and medical journals. This month, the following topics are explored:
Having Hepatitis B and a Family Member with Cancer Raises Cancer Risk Dramatically
VA Tests Only 21.8% of Its Patients for Hepatitis B, Missing Many at Risk of Infection
Research Shows Importance of HBV Screening Before Chemotherapy Begins
Younger Age and Low HBsAgLevels Benefit Patients Who Stop Antivirals
Doctors Debate Benefits of Interferon vs. Antiviral Treatment
New Study Finds Fibroscan Accuracy on Par with Liver Biopsies
Mild Kidney Problems and Bone Loss Linked to Antivirals
Hepatitis C is now declared curable. Hepatitis B is still not, despite having been discovered nearly 50 years ago. An interview with Dr. Timothy Block of the Hepatitis B Foundation and the Baruch S. Blumberg Institute. The future does look bright…
Perhaps this should not be a surprise, thinks Timothy Block, PhD, president and co-founder of the Hepatitis B Foundation (HBF) and its research arm, the Baruch S. Blumberg Institute. According to Block,there are two main reasons for the “cure deficit” between hepatitis B and C — funding and physiology.
He points out that commercial and federal investment in hepatitis C have been far greater than in hepatitis B. And that has clearly paid off in terms of finding a hepatitisCcure. “You get what you pay for,” he observes.
Physiologically,hepatitisB also presents unique challenges not found with hepatitisC — most notably cccDNA (or covalently closed circular DNA), the “mini- chromosome” produced by the hepatitis B virus. The cccDNA persists in the nucleus of the liver cell, where it can hide amidst the host’s own chromosomes, apparently out of reach of the cell’s own defense systems.
Acting like “an indestructible template,” cccDNAcontinues to produce virus particles throughout the life of the infected liver cell, even in people being treated with antiviral agents.
Hepatitis C, on the other hand, doesn’t enter the cell’s nucleus, so it’s possible to cure a person by stopping this virus from replicating long enough for the liver cells to regenerate.
But remember that people who have been “cured” of hepatitis C can still get re-infected,” Block cautions. The hepatitis C drugs apparently do not trigger an immune response that protects against re-infection.
In contrast, some people can be cured of hepatitis B, either naturally or through drug therapy. These individuals do seem to have long-term protective immunity. “And that’s what we are aiming for,” he declares.
Why We Need a Cure for Hepatitis B
It can be argued that the approved antiviral agents are very successful in keeping the virus under control. So do we really need a cure? Definitely yes, Block replies emphatically.
Current antiviral drugs are effective, but need to be taken lifelong and are recommended for use in only about half of the infected population. And even after 10 years of use, the antivirals reduce HBV-related diseases by only about 50 to 60 percent. The drugs can also lead to the development of resistant hepatitis B strains (drug resistance).
For those who benefit from treatment, the antiviral drugs have been transformational and prove that medical intervention can be effective. However, there are millions who do not benefit and are still left vulnerable.
Clearly, new approaches to a “functional cure” are needed, which Block defines as “returning the risk of death due to hepatitis B to the level of someone who has a resolved infection.” And the person should not need to take any drugs to stay at this low-risk level.
Targeted Strategy for a Cure
The HBF/Blumberg Institute scientists, with their research partners from Drexel University College of Medicine, both located in the HBF’s Pennsylvania BiotechnologyCenter, are developing two types of therapies: direct-acting antivirals and innate host defense activators. The first type inhibits virus-host interactions and viral gene products; the second recruits the host’s immune system to attack and eliminate cccDNA and infected liver cells.
For each of these approaches, the researchers have identified key steps to target in the hepatitis B infection cycle, from virus entry into the liver cell, to cccDNA replication, to formation of virus particles.
For many of these steps, “Our scientists have developed assays that can be used to screen for new drugs. We are a recognized leader in designing and developing these assays and, for a time, had the only cccDNA- dependent cell lines,” notes Block. Almost 100 different cell lines for assays have been developed that can be used to screen for drugs that activate the innate host defense pathways.
For drug screening, cell lines are incubated with potential drug candidates to try and find new therapeutic drugs for future hepatitis B treatment. The strategic goal is to discover new drugs that complement existing therapies, but also enable the immune system to provide long-lasting antiviral protection, even when the person is no longer on drug therapy.
The strategic goal is to discover new drugs that complement existing therapies, but also enable the immune system to provide long-lasting antiviral protection, even when the person is no longer on drug therapy.
Several compounds in development already show some effectiveness in animal models. “We have a capsid inhibitor, a pregenomic RNA capsid inhibitor (JT Guo), an HBsAg inhibitor (A Cuconati), a cccDNA repressor (H Guo, A Cuconati, JT Guo), and an activator of innate host defense pathways (J Chang and JT Guo),” Block reports.
He is particularly excited about their stimulator of interferon genes (STING) agonist, which was very effective in mouse models. The research group is now working on a human STING agonist, although an appropriate assay for this compound still needs to be developed.
What the Future Holds
“The Hepatitis B Foundation and its Blumberg Institute have contributed
to some of the most important work in studying the phases of the virus lifecycle that has led to the currently available drugs. Our researchers continue to be at the forefront in developing a promising pipeline for hepatitis B drug discovery,” says Block.
“I am absolutely confident that a cure is possible” he asserts. “After all, enough people with hepatitis B resolve their infections, either medically or spontaneously — even some people with chronic infections. So we know it’s possible.”
The World Health Organization (WHO) will release their first management guidelines for hepatitis B virus (HBV) by the end of 2014. For the first time, the guidelines will be geared towards resource-constrained countries, where the disease burden is high but resources are lacking. The new guidelines will be particularly welcome in African nations, where the incidence of viral hepatitis is increasing.
The overall scope of the World Health Organization’s new management guidelines for hepatitis B will include prevention, screening, and treatment of chronic hepatitis B and will be geared towards resource-constrained countries. Thus, WHO’s guidelines will be valuable for countries where the disease burden is high but resources are lacking.
The new WHO guidelines will be particularly welcome news to African nations, where the incidence of viral hepatitis is increasing.
According to the WHO Global Hepatitis Survey 2013, the prevalence of chronic hepatitis B virus (HBV) infection on the African continent is up to 8% of the general population, and 75% of the population may have had prior exposure to the virus.
Yet, only two of the African member states that responded to the WHO Survey have a written national strategy to prevent and control viral hepatitis.
In Ghana, where the incidence of viral hepatitis is increasing, the sero-prevalence rate is high among blood donors (6.7%), pregnant women (6.5%) and school
aged children (15.6%), according to Mr. Theobald Owusu-Ansah, president of the Theobald Hepatitis B Foundation and the Hepatitis B Coalition in Ghana.
Compounding the lack of public health plans and national investment are factors common in many low-resource countries: limited awareness of hepatitis B among the public and providers, poor access to care, expensive therapies, and few liver specialists.
Global agencies are beginning to recognize the urgency of the situation. In addition to the WHO, the World Health Assembly is taking steps to combat the growing crisis. The Assembly adopted a second resolution on viral hepatitis in May 2014 that advises governments on how to prioritize and coordinate public health efforts.
But governments cannot tackle these problems alone, Mr. Owusu-Ansah believes. He urges governments to partner with commercial and nonprofit organizations to mobilize much-needed expertise and resources.
HBF is pleased to connect our blog readers to Christine Kukka’s monthly HBV Journal Review that she writes for the HBV Advocate. The journal presents the latest in hepatitis B research, treatment, and prevention from recent academic and medical journals. This month, the following topics are explored:
Twenty-five Percent of HBV-Infected Women Have Liver “Flares” after Childbirth
Experts: Do Not Treat Patients in the Immune-Tolerant Stage of Infection
Entecavir and Tenofovir Equally Effective in HBeAg-positive Patients and Cirrhotics
Tenofovir Effective in Patients with Adefovir- and Lamivudine-Resistance
Adding Interferon to Ongoing Antiviral Treatment Effective in HBeAg-positive Patients
Antivirals Improve Survival Among Hepatitis B Patients
Interferon Effective in HBeAg-negative Patients, Early HBsAg Declines Predict Success
Study Finds Asian Immigrants, Especially Chinese, at High Risk of Hepatitis B
Immunization Continues to Protect Against Hepatitis B Decades Later
Doctors Fail to Vaccinate Hepatitis Patients Against Other Hepatitis Infections
Study Confirms HBV Patients Have Higher Kidney Disease Rates
Get HBV Advocate’s Christine Kukka’s take on the top HBV related, published reports from the AASLD Liver Meeting as she provides her Top Ten List!
Top Ten Reports from the 65th Annual Liver Meeting By Christine M. Kukka, HBV Advocate
Hepatitis B experts from around the world met at the 65th annual American Association for the Study of Liver Diseases (AASLD) conference in Washington D.C. this week to share the latest in hepatitis B treatment and research.
Which combination of antivirals and interferon works best against hepatitis B
Tenofovir continues to excel with no signs of drug resistance after eight years
Tenofovir treatment is safe over an entire pregnancy for both mother and child
Tenofovir and entecavir combination successful against drug-resistant HBV
Who remains at risk for hepatitis B in the U.S.?
Antivirals appear to lower liver cancer risk
But antivirals don’t reduce cancer risk in older patients with cirrhosis
How long do patients have to keep taking antivirals after they lose HBeAg and achieve undetectable viral load?
Liver cancer risk remains, even after HBsAg clearance in older, male patients
Experts say treatment is needed when ALT levels are only moderately elevated
HBF is pleased to connect our blog readers to Christine Kukka’s monthly HBV Journal Review that she writes for the HBV Advocate. The journal presents the latest in hepatitis B research, treatment, and prevention from recent academic and medical journals. This month, the following topics are explored:
Experts Say Breastfeeding While Taking Antivirals Is Safe
Doctors Fail to Adequately Treat HBV-Infected Women After Childbirth
Doctors Continue to Fail to Screen Asian-Americans for Hepatitis B
Statins Protect Hepatitis B Patients Against Heart Disease and Liver Cancer
New Study Finds Antivirals Lower Liver Cancer Risk
Studies Find Tenofovir Lowers Viral Load Faster Than Entecavir
Liver Transplants Safe in Older Hepatitis B Patients
Scientists Develop Micro Weapon to Disable HBV’s Cancer-Causing X Protein
Foreign-Born U.S. Residents Less Likely to Be Immunized
Antivirals Can Safely Replace HBIG Following Liver Transplantation
All Hepatitis B Patients Appear at Risk from Chemotherapy
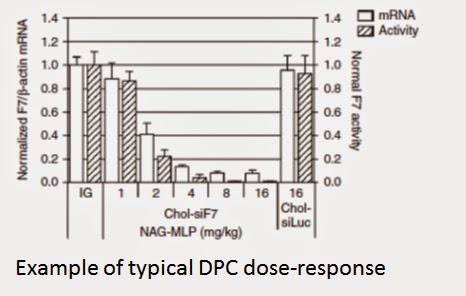
It should be noted while numerically the improvement in knockdown from 1mg/kg to 2mg/kg was only 12%, this is likely the result of the apparent high variability at the lower dose level with the increased tightness of the knockdown range at 2mg/kg indicating that the RNAi mechanism is starting to be solidly engaged with the expectation of a steepening dose response going forward.
Sadly, we read that Phase 2a data presented by Arrowhead fell short of expectations for their ARC-520 drug to treat chronic hepatitis B. Hopefully dose escalation to 4mg/kg will result in both effective and safe results. However, there are others in the race for the cure, and may the most effective and safe drug soon result in a functional cure for chronic HBV.
~ hepbtalk
Harnessing the Power of RNAi Gene Silencing in Quest of a Cure for Chronic Hepatitis B, and the HBV KnockDown blog written by Dirk Haussecker, who believes it’s about time everyone got serious about a functional cure for hepatitis B. Be sure to visit Dirk Haussecker’s blog !
Today, we learned about some hard HBsAg knockdown numbers from the phase IIa Hong Kong study of ARC520 in chronically infected HBV patients. The data relate to the first 2 cohorts in this ongoing dose escalation trial. Accordingly, the mean HBsAg knockdown at nadir for the starting dose of 1mg/kg was 39% within a range of 22-57%(n=6) while it was 51% within a range of 46-59% for the 2mg/kg cohort (n=6).
ARC520 was given as a single dose to patients already stably on polymerase inhibitor entecavir.
While clearly missing the company’s own guidance of a 1 log reduction at 2mg/kg, the good safety profile-no SAEs at all in the study with all AEs rated to be unrelated to ARC520- in addition to the steepening dose-response curve following 2mg/kg means that ARC520 is far from being out of the HBV knockdown race. Still, the stock market over-reacted, punishing ARWR stock with a percent decrease that matched the reported knockdowns.
Although even I ended up willing myself into believing that a 70-80% knockdown was possible following a single ARC520 dose of 2mg/kg, revisiting the chimp study which involved 2 doses of ARC520 (first one at 2mg/kg then one at 3mg/kg), it should be noted that at the time the 3mg/kg dose was administered, the HBsAg levels had only declined by 50%…about the same as achieved in the phase IIa study. It is thus possible that Arrowhead gave the 2nd dose just as HBsAg levels were about to go up again, consistent with the already rebounding levels of HBV DNA and HBeAg in that study.
As a result, my expectations for the single 3mg/kg dose are now 70-75% based on the ~75-80% peak HBsAg knockdown in the chimp study following the 2mg/kg and 3mg/kg doses. This also means that in order to reach that 1log knockdown goal the company had set for itself, 4mg/kg will most likely be needed. Importantly, in the concurrent phase I dose-escalating study in healthy volunteers, this quite large amount of drug seemed to be well tolerated and the company is awaiting approval to adopt this dose in the Hong Kong study.
This projection is not much off the 90% knockdown achieved in the ARC-AAT program at 3mg/kg in non-human primates. The improvement of this 2nd DPC-based candidate about to enter the clinic is possibly explained by progress in the potency of 2-molecule DPC delivery technology. I add this as today many were confused about what the interim phase IIa results meant for the platform and the value of the company.
Overall, as long as 4mg/kg is an acceptable dose from a tox point-of-view, ARC520 is still in the game to be first-in-class in HBV knockdown. It would have been much worse if say a 70% knockdown had been reported, but worrisome safety signals emerged. On the other hand, the continued need for a dose escalation would seem to delay Arrowhead’s broad-based phase IIb study plans, meaning that the competition, in particular Tekmira’s TKM-HBV is coming closer.
At a market cap of ~$400M, the market has almost fully discounted the potential of ARC520 given the $150M+ in cash as well as the IND-ready, first-in-class ARC-AAT for which we can expect solid knockdowns in the clinic. Interestingly, data for this candidate were selected for an oral presentation at AASLD while the ARC520 data will be in less prestigious poster form. Finally, should the single-molecule DPC which got me excited about the Arrowhead RNAi platform in the first place finally reach the clinic, it would necessitate an upward revision of the value of the company.
Disclosure: Long ARWR. I sold most of my holdings at $11 and change given the underwhelming results and increasingly negative market reaction, but got back in below $6 when I considered the sell-off to be a gross over-reaction and imminent 3mg/kg data having the potential to surprise the market to the upside from now much lowered expectations. Add to this ARC-AAT, the platform…
HBF is pleased to connect our blog readers to Christine Kukka’s monthly HBV Journal Review that she writes for the HBV Advocate. The journal presents the latest in hepatitis B research, treatment, and prevention from recent academic and medical journals. This month, the following topics are explored:
Chronic Hepatitis B Remains Public Health Challenge in U.S.
Epidemiologists Become Molecular Detectives to Investigate HBV Outbreaks
Telbivudine Effectively Prevents Infection of Newborns Born to Infected Mothers
GGT Blood Test Reveals Fibrosis and Cirrhosis in Hepatitis B Patients
Early Research Combining Antivirals with a Protein “De-activator” Shows Promise
Diabetes Dramatically Increases Liver Cancer Risk in Cirrhotic Patients
Tenofovir Linked to Higher Rates of Bone Loss than Entecavir
Tenofovir Equally Effective against Hepatitis B in Asians and Non-Asians
Liver Cancer Risk Factors Do Vary Between Racial Groups
Even Liver Specialists Fail to Screen Chemotherapy Patients for Hepatitis B
European Study Confirms Coffee Dramatically Lowers Liver Cancer Risk
HBV Journal Review
October 1, 2014
Volume 11, Issue 10 by Christine M. Kukka
Chronic Hepatitis B Remains Public Health Challenge in U.S.
A new U.S. Centers for Disease Control and Prevention report on hepatitis B prevalence finds that while new infections have declined markedly, treating chronic hepatitis B infection remains a public health challenge.
New hepatitis B virus (HBV) infections have plummeted since 1990 due to comprehensive immunizations. The CDC report estimates only 18,760 people were infected with HBV in 2012.
In 2012, the highest rates of new infections were among those aged 30–39 years (2.17 cases per 100,000 population), and the lowest were among children under age 19 who had been immunized at birth.
Many of the new infections were transmitted sexually or through injecting drug use.
However, an estimated 700,000 to 1.4 million U.S. residents are chronically infected. According to the report, Viral Hepatitis Surveillance United States, 2012, about half of those chronically infected were either born in Asia or were born to HBV-infected mothers in the United States.
In 2011, the death rate from chronic hepatitis B was 0.5 deaths per 100,000 population. The highest mortality rates were among people aged 55–64 years, Asian and Pacific Islander, and male.
“Identifying these chronically infected persons and linking them to care remains a challenge,” the authors reported.
Epidemiologists Become Molecular Detectives to Investigate HBV Outbreaks
While new HBV infections have declined dramatically since the early 1990s due to effective immunizations, public health officials continue to examine where new infections are coming from and who is getting infected.

 HBF is pleased to connect our blog readers to Christine Kukka’s monthly HBV Journal Review that she writes for the HBV Advocate. The journal presents the
latest in hepatitis B research, treatment, and prevention from recent academic and medical journals. This month, the following topics are explored:
HBF is pleased to connect our blog readers to Christine Kukka’s monthly HBV Journal Review that she writes for the HBV Advocate. The journal presents the
latest in hepatitis B research, treatment, and prevention from recent academic and medical journals. This month, the following topics are explored: