Welcome to “Journey to the Cure” This is a web series that chronicles the progress at the Hepatitis B Foundation and Baruch S. Blumberg Institute towards finding the cure for hepatitis B.
In the second episode (part 1), Kristine Alarcon, MPH sits down with Chari Cohen, DrPH, MPH, Vice President of Public Health of the Hepatitis B Foundation, to talk about hepatitis B symptoms and testing.
For any questions about hepatitis B, please email info@hepb.org
The Hepatitis B Foundation is a national nonprofit organization dedicated to finding a cure and improving the lives of those affected by hepatitis B worldwide through research, education and patient advocacy. Visit us at www.hepb.org, on Facebook at www.facebook.com/hepbfoundation, on Twitter at @hepbfoundation, and our Blog at www.hepb.org/blog
Disclaimer: The information provided in this video is not intended to serve as medical advice or endorsement of any product. The Hepatitis B Foundation strongly recommends each person discuss this information and their questions with a qualified health care provider.
Diabetes is a chronic condition that is characterized by high glucose (or sugar) levels in the blood. It usually occurs when a person cannot produce enough insulin, a hormone that controls blood sugar levels. According to the World Health Organization (WHO), global prevalence of diabetes is on the rise! In 1980, diabetes prevalence in adults over the age of 18 was 4.7%. The number rose to 8.5% in 2014 and continues to increase. In 2015, there was an estimated 1.6 million deaths that were attributed to diabetes.
Like hepatitis B, there have been several studies that show a strong link between type II diabetes and liver cancer. Diabetes and hepatitis B can be a dangerous combination and can work together to increase someone’s risk of developing liver cancer.
Since the hepatitis B virus can be transmitted via blood or other bodily fluids, people living with diabetes are at an increased risk of contracting hepatitis B. In fact, one study found that people living with diabetes between the ages of 23-59 have an approximately two-fold increased risk of hep B infection compared to those without diabetes. According to the Centers for Disease Control and Prevention (CDC), there have been hepatitis B outbreaks in nursing homes, assisted living, and long-term care facilities among people living with diabetes. Some risks for transmission include:
Sharing glucose meters between residents without cleaning and disinfecting between uses
Lack of proper hand hygiene and failure to wear gloves between fingerstick procedures
Using the same fingerstick devices for more than one resident
Cross-contamination of clean supplies with contaminated blood glucose monitoring equipment used by home health agencies
Sharing injection equipment such as an insulin pen or syringe for more than one person
Failure to perform proper sterilization and separating contaminated and clean podiatry equipment
Failure to perform proper disinfection between podiatry patients
So, what can you do if you are living with diabetes to prevent hepatitis B transmission?
Get tested! A simple three-part blood test will tell you if you have hepatitis B, were exposed, or are protected.
Get vaccinated – If you find that you are not protected or if you have not finished your hepatitis B vaccine series. The CDC and Advisory Committee on Immunization Practices (ACIP) recommend that adults between 19-59 years of age living with diabetes get vaccinated to protect against hepatitis B. Those 60-years-old or older should ask their doctor about the vaccine before getting it.
Do not share your diabetes care equipment to prevent exposure!
Around the world, the most common mode of hepatitis B transmission is from mother to child. Unfortunately, pregnant mothers who have hepatitis B can transmit the virus to their newborn during the delivery process. 90% of these HBV infected babies will progress to chronic infection putting them at increased risk of serious liver disease or liver cancer later in life.
It is important that ALL pregnant women get tested for hepatitis B to prevent the transmission of the virus to newborns at birth.
The U.S. Centers for Disease Control and Prevention (CDC) recommends that all newborns born to hepatitis B positive women be given two shots in the delivery room – the first dose of hepatitis B vaccine (5 mcg dose) and one dose of hepatitis B immune globulin (HBIG, 0.5 mL dose). If a woman knows that she is infected, it is important that she tell her doctor to have these two drugs available when she is ready to deliver. These two shots must be given at separate injection sites, i.e. different limbs. When administered correctly within the first 12 hours of life, a newborn has a 95% chance of being protected against a lifelong hepatitis B infection. The infant will need to complete the hepatitis B vaccine according to schedule as part of a 3 or 4 dose series. CDC recommends follow up testing to confirm immunity or protection against HBV at 9 months or at the baby’s 1 year checkup.
The World Health Organization (WHO) recommends the birth dose of the hepatitis B vaccine for ALL babies, though it is especially important for a baby born to a woman with hepatitis B to receive the first dose of the vaccine as soon as possible, within 24 hours. HBIG may not be available in all countries or may be cost prohibitive. The hepatitis B vaccine series may be completed with the remaining monovalent (single) injections of the HBV vaccine, or may be completed as part of a combination vaccine series.
In developing countries combination vaccines such as the pentavalent vaccine are often given to babies. The first dose of the pentavalent vaccine (which includes hepatitis B vaccine) is given at 6 weeks of age, and the 2nd and 3rd doses are given at 10 and 14 weeks of age. Waiting for the first dose at 6 weeks is too late for babies born to mothers living with chronic hepatitis, though the pentavalent vaccine should never be used as the birth dose or before 6 weeks. Women who know they have hepatitis B should talk to their doctor about ensuring that a birth dose of the hepatitis B vaccine is available for their baby at birth.
There is no second chance! It is vitally important that we protect all newborns from hepatitis B!
Also, all infected pregnant women need to learn more about their hepatitis B infection from a liver specialist or a doctor with experience treating patients with chronic hepatitis B. It is recommended that pregnant women have their hepatitis B monitored throughout their pregnancy, to check the health of their liver and to see if they need treatment. For HBeAg positive women with high hepatitis B viral loads, taking FDA-approved antivirals during the last trimester can reduce the amount of virus in the blood and help prevent the chance of transmission to the newborn. Once an infected woman gives birth, it is important that she routinely see her doctor to keep monitoring her hepatitis B infection. Keeping mothers healthy allows them to better take care of their families!
For more information, or if you live in the U.S. and need help with hepatitis B infection during pregnancy, please visit the Perinatal Hepatitis B Prevention Program to find a coordinator near you. If you are outside of the U.S., you may consider visiting the World Hepatitis Alliance to find if there are organizations in your country that can ensure your baby starts with a birth dose of the hepatitis B vaccine.
Around the world, millions of people with chronic hepatitis B face wrenching discrimination that limits their dreams, education, careers, income and personal relationships.
Discrimination is unethical, unnecessary and a violation of human rights. Hepatitis B is simply not transmitted through casual contact. The stigma that persists is based on ignorance and it impacts millions around the world daily. The United Nations created Zero Discrimination Day to highlight the negative impact of discrimination and promote tolerance, compassion and peace. Many hepatitis activist organizations, including the Hepatitis B Foundation, used this commemorative day to draw attention to global hepatitis B discrimination. Even though Zero Discrimination Day was on March 1, we still need to recognize the importance of stopping hepatitis B discrimination.
Every day is zero discrimination day, and ending discrimination starts with each of us working in any way we can in our communities to end this stigma.
No one is to blame for hepatitis B, and people who have hepatitis B deserve the same opportunities to live fulfilling lives – at work, at home and in the community. . There is a safe and effective vaccine that prevents hepatitis B infection. When people are protected, there is no reason to fear that healthcare workers or hotel maids will spread this infection. Even without vaccination hepatitis B transmission can be avoided with simple prevention measures. Hepatitis B is not transmitted casually.
People who have hepatitis B are part of our global community. They are our mothers, brothers, doctors, teachers, spouses and friends. To learn about how the fear of discrimination affects people who have hepatitis B, check out some of our #justB patient stories. Jin’s story tells us how a vibrant young woman handles her fear, and Carolyn’s story shows us the devastating consequences of hiding a hepatitis B diagnosis.
It is morally reprehensible that given the tools and knowledge we have that discrimination against people who have hepatitis B should continue today. So we ask you to help us end this discrimination.
One way you can fight hepatitis B discrimination is by joining the World Health Alliance in their #StigmaStops awareness campaign. It is a year-long campaign that highlights the stigma and discrimination associated with hepatitis around the world. #StigmaStops provides people living with hepatitis a platform to strengthen their voice and speak about the stigma and its impact as well as dispel myths and misconceptions of hepatitis B. Another way to help is to talk about hepatitis B – with your colleagues, friends and family members. The more we talk openly about hepatitis B, the less it will be stigmatized. And feel free to share our #justB videos – they can be a great conversation starter!
Welcome to “Journey to the Cure” This is a web series that chronicles the progress at the Hepatitis B Foundation and Baruch S. Blumberg Institute towards finding the cure for hepatitis B.
In the first episode (part 2), Kristine Alarcon, MPH sits down with Timothy Block, PhD, President and Co-Founder of the Hepatitis B Foundation, to talk about what a hepatitis B cure could look like in the future.
For any questions about hepatitis B, please email info@hepb.org
Disclaimer: The information provided in this audio post is not intended to serve as medical advice or endorsement of any product. The Hepatitis B Foundation strongly recommends each person discuss this information and their questions with a qualified health care provider.
Special Thanks:
Samantha Young
Music:
Modern – iMovie Library Collection
Script:
Welcome to Journey to the Cure! Every month, we’ll sit down with scientists from the Hepatitis B Foundation and the Baruch S. Blumberg Institute to talk to you about hepatitis B and efforts to find a cure for hepatitis B. There’s still a long way to go, but we’re here to walk you through our journey.
Timothy Block, PhD:
The Hepatitis B Foundation is now largely devoted to basically outreach and what I call human services or being there for people. We wanted, however, to keep pressure on research communities – to make sure there was a research organization. The Hepatitis B Foundation created a second non-profit organization, originally called the IHVR, renamed in Dr. Blumberg’s honor after he passed away; and that’s the Baruch S. Blumberg Institute. And that’s a group of research scientists.
Kristine Alarcon, MPH:
What do we need in order to find a cure for hepatitis B?
Timothy Block, PhD:
Well, we need more research. We need focused research and the community’s kind of coming together with a consensus. The Hepatitis B Foundation organized that workshop, which we published research priorities. We call it the “Roadmap to a Cure.” The more scholarly, conservative title for that is a research agenda- research priorities. We believe that if you follow that roadmap or you follow those lists, we will be most likely- I don’t want promise anything- but we will most likely to find if not a cure, transformational new medicines. But, I’m hopeful that they’ll be one form of cure. So you follow that roadmap, and we should get there.
Kristine Alarcon, MPH: Thank you so much. This has been very insightful on what it looks like for the cure in the future. Thank you again for joining us.
Timothy Block, PhD:
Thank you again so much for the opportunity and what I want the listeners to know that the Hepatitis B Foundation is at the forefront of this work. We were there 27 years ago. We were there through the times when hepatitis B was being forgotten. The cure for hepatitis C has brought new focus on the problem of hepatitis and we were- and we’re here now. We’re sitting in an office that is in a building that has the Hepatitis B Foundation outreach and advocacy staff of nurses and public health professionals. We’re also here with as I said with 100 scientists, who are focused on looking for a cure for hepatitis B. We’re working for the commercial community, working with the academic community. But we’re here stimulating the research, promoting workshops, promoting seminars, but also doing our own research. So I hope that you keep that in mind and know that there are- there are a group of people who remain very focused on it.
Kristine Alarcon, MPH:
Thank you so much for joining us and we’ll see you on the next episode.
Join Kristine Alarcon, MPH for A Day in the Life of a Public Health Coordinator to learn about some of the activities we at the Hepatitis B Foundation take part in!
This episode highlights our events for our local program, Hep B United Philadelphia, during January 2018. We show you the “behind-the-scenes” of a hepatitis B screening event.
Hepatitis B Foundation Health Outreach Coordinator and Guest Blogger Sierra Pellechio, B.S., CHES discusses her work with the African Immigrant community.
Hepatitis B affects over 2 million people in the United States, disproportionately affecting Asian, Pacific Islander and African Immigrant (AI) communities in the U.S. Although partners around the U.S. have been trying to increase awareness and improve screening and linkage to care rates among high risk communities, there have been few programs designed to address the urgent need for intervention among U.S. AI communities. An estimated 5% to 18% of African immigrants in the U.S. are affected by hepatitis B, with less than 20% aware of their infection. However, since research and prevalence data specific to AIs are lacking, it has been difficult to understand the true burden of this disease. One thing we do know is that there are significant knowledge gaps and low screening and linkage to care rates in AI communities. If left undiagnosed, people with hepatitis B are at risk of developing liver complications, including cirrhosis and liver cancer, which can lead to premature death, making it vital to identify those affected. This is complicated by the fact that hepatitis B is a silent disease with few or no symptoms for decades.
Working with a diverse sixteen-member expert advisory committee comprised of African community leaders, providers, and public health experts from across the U.S., the first phase of this project assessed the individual, community, and society-level barriers that affect hepatitis B screening, vaccination, and linkage to care. Findings revealed that a potentially effective strategy for improving awareness and testing could involve first educating community health workers, who would then serve as trusted educators and advocates to promote education and testing in their communities. In collaboration with the advisory committee, the Hepatitis B Foundation is developing two training modules tailored to community health workers. The modules focus on providing basic hepatitis B information, addressing myths and stigma, and suggesting strategies for incorporating health messages into their work that are culturally and religiously relevant. These educational modules will have an accompanying audio recording, a comprehensive resource guide, and a flipchart for direct community education on hepatitis B. To ensure relevance and effectiveness, these materials will be pilot tested and revised prior to nationwide dissemination. Once the project concludes, resources and materials will be available on the Hepatitis B Foundation and CDC resource pages in early 2019.
If you are a community health worker working in the African Immigrant community and would like to connect, share resources, or learn more, please contact the manager of this project, Sierra Pellechio at sierra.pellechio@hepb.org.
Happy Valentine’s Day!! Today is dedicated to celebrating love. Though it can be exciting, anxiety can creep up on this day too. Maybe you’re thinking about confessing your feelings to your crush? Or nervous about planning the best date ever? Maybe you’re timid about the holiday in general because of your hepatitis B status?
If you have chronic hep B, you may think that starting a relationship and initiating sex can be stressful and feel overwhelming. Questions like “What if we break up because I disclosed my status?” or “Can I even start a relationship with someone if I have a chronic disease like hepatitis B?” may be swimming in your mind. Doubt and anxiety may overwhelm your thoughts, but don’t forget that you’re more than your illness. You should not focus on things you cannot change. You are worthy of love and can live out that romantic story you always wanted because you have wonderful things to offer to a future love interest.
If you’re spending time with someone on Valentine’s this year or any day, it’s important that you remember to take precautions if your date leads to an intimate night. If you are living with hep B, properly wearing a latex condom keeps you safe from becoming co-infected with another infectious disease. No one wants a co-infection. It is complicated and potentially dangerous for you and your partner’s health. If your partner does not have hep B, then avoid infection by wearing a condom. Hep B is vaccine preventable, but hepatitis C, HIV and other sexually transmitted infections (STIs) are not. Considering the health and safety of yourself and your sexual partners is paramount. You may not know what they have, and they may not know what you have.
Also, it is important to disclose your status before sex (even if it’s safe sex with a condom). You may jeopardize your partner’s trust (and their health) before the relationship deepens. Disclosing your chronic hep B status can be scary, but talking about it reduces the stigma surrounding the infection and may even prompt your partner to get tested or vaccinated if needed. If your partner is not understanding after you have explained your HBV infection, then you know that person was not meant for you, and not deserving of your love. There are other potential partners out there that will be understanding and loving. Do not let rejection discourage you!
Disclosure should be done calmly and carefully. It is important to do some research before you do disclose your hepatitis B status. Having a thorough understanding of hepatitis B can make it easier for you to explain it to a future partner. The more you know, the less scary and more comfortable it is to dispel fear, so that you can share your status with confidence and integrity.
Whether you think of today as Valentine’s or Single Awareness Day, remember that hep B is only a small part of who you are and should not be a reason for you to give up on loving someone. Remember that you are more than your chronic hep B! It’s only a part of you and does not define your entire life. You have so much to offer to your current or future partner!
Have you been thinking about adoption for a long time or have been inspired by NBC’s show, This is Us, to adopt? Adoption is exciting! However, it can be nerve wracking and feel overwhelming. We at the Hepatitis B Foundation can help with one aspect of the adoption process – making sure you have accurate information about hepatitis B.
It is important to be armed with accurate information about hepatitis B when preparing for adoption for both international and domestic adoptions. This can help protect your future child, family members and yourself when you welcome your future child with open arms.
Many people wish to adopt children from countries where hepatitis B infections are common: Asia, South America, Eastern Europe, and some parts of Africa. Children from these regions could be infected with the virus since it can be unknowingly passed from birth mothers who have hepatitis B and transmit the disease to their children during delivery. In addition, many of these countries struggle with proper infection control practices that place babies and young children at risk with unsafe medical procedures. Unfortunately, many infants still do not have access to the birth dose of the hepatitis B vaccine to help prevent transmission.
Domestic adoptions also present some risk. Children born to women in high-risk groups (e.g. illicit drug users, multiple sexual partners, etc.) could be exposed to hepatitis B at birth. In addition, children from group homes are at increased risk for hepatitis B infection. The good news is that there are procedures in place that can prevent a baby from getting infected if born to an infected mother – and the success rate is up to 95%! This includes providing the first dose of the hepatitis B vaccine along with a dose of hepatitis B immune globulin (HBIG) within 12 hours of birth. If you are planning a U.S. adoption, and know that the birth mother is infected, you can ensure that the birth hospital knows about these procedures and can administer the shots on time.
During the adoption process, the adoption agency should tell you if your child has been tested for hepatitis B, but there can be errors if the child was tested only as an infant. With an international adoption,it is advised that you do not request that your child be tested since the blood test itself could be a source of infection. If you are concerned about the results of these tests, please contact us to speak with our knowledgeable staff. We can also refer you to a parent who has adopted a child with hepatitis B. Whether your child has been diagnosed with hepatitis B or not, testing for HBV should be repeated once you’re home. If needed, you can refer to our physician directory to find a pediatric specialist who knows about hepatitis B.
If you do find out that your child does have hepatitis B, you can handle it!Hepatitis B is a manageable disease. Many families seeking a “special needs adoption” choose to adopt a child with chronic hepatitis B because it is manageable and treatable. Hepatitis B is a vaccine preventable disease, so newly adopted children can be safely integrated into vaccinated families. Children with chronic HBV can expect to live a long and healthy life if they are monitored by a pediatric liver specialist. Some may need treatment during childhood, most probably won’t. Hepatitis B does not affect a child’s growth and development, and there are generally no restrictions associated with chronic hepatitis B. It is recommended that those with chronic hepatitis B see a pediatric liver specialist every six months for hepatitis B management. Often this entails only blood work to monitor the child’s HBV and liver health. Also make sure household members are vaccinated and that you talk to talk to all of your children about the importance of handwashing and “never touching anyone’s blood”. When your children get older, help them acclimate to dating and disclosure. The hepatitis B vaccine is required for school in all but four states.
For some tips, you can visit our website on adoption, children with hepatitis B, and one of our previous blogs. You can also watch some adoption stories from our #justB storytelling campaign. Be sure to watch Maureen’s, Maureen K’s, and Jin’s stories about the international adoption process with hepatitis B. You can also watch Janet and Kurt’s domestic adoption process. Please consider opening your home to an adopted child. It will change your life.
Did you know that the hepatitis B virus doesn’t just infect humans? It also infects chimpanzees1, tree shrews1, Peking ducks1, horses2, and woodchucks2. The hepatitis B virus that infects woodchucks is closely related to the human hepatitis B virus.2 Because of this, woodchucks have been a prominent animal model in studying the hepatitis B virus and testing drugs for the disease.2,3
Behind every legacy, there is a man who started it all. In the case of the woodchucks and hepatitis B, there was Bud Tennant, DVM. Dr. Tennant was a California native, born in the San Joaquin Valley.2 He studied veterinary medicine, earning his Doctor of Veterinary Medicine from the University of California at Davis in 1959. 2 As a veterinarian, Dr. Tennant conducted research in comparative medicine focusing on hepatocarcinogenesis (development of liver cancer), hepatic injury mechanisms, viral hepatitis, and gastrointestinal and liver diseases of domestic animals.2
His work in hepatitis started during his tenure as the James Law Professor of Comparative Medicine at Cornell University, where he studied the pathogenesis of serum hepatitis in horses.2 He would not work with woodchucks until Dr. Norman Javitt, Chief of Gastroenterology at Weill-Cornell Medical College at the time, approached him, urging the need for an animal model for studying hepatitis B virus to understand pathogenesis, treatment, and prevention of hepatitis B. Dr. Javitt introduced him to Drs. Jesse Summer and William Mason’s research on a new virus infecting woodchucks, its close relation to human hepatitis B virus, and its association with chronic hepatitis B and liver cancer.
Dr. Tennant spent over thirty years on the study of Woodchuck Hepatitis Virus infection, working with a colony of woodchucks in Ithaca, New York. 2 He developed the woodchuck as a successful animal model to learn how hepatitis B effects the liver, including the development of liver cancer. His work with the woodchuck model ultimately enabled scientists to run clinical therapeutic trials for treating hepatitis B in humans. 2 In fact, preclinical studies for almost every hepatitis B therapeutic drug licensed by the FDA have been conducted using the woodchuck model! Today, the Woodchuck Hepatitis Virus infection study continues at the Roswell Park Cancer Institute in Buffalo, New York. 2
Dr. Baruch S. Blumberg would also contact him to work together on fighting the hepatitis B virus in humans.
Dr. Bud Tennant is famous in the scientific world for his game-changing work in hepatitis B, and won many awards. At the 2016 Hepatitis B Foundation Crystal Ball, Dr. Tennant was presented with the 2016 Baruch S. Blumberg Prize, the Foundation’s highest honor. 2 He was also beloved by those who worked with him. He was known as “a towering physical presence, yet soft spoken and humble, and he was greatly admired for his good nature and his ability to share a story on just about any topic.” 2 Though Dr. Tennant passed away in 2016, he will always be remembered for his unwavering commitment, and thought of as a valued friend and mentor to many scientists. 2
References:
Schinazi, R.F., Ilan, E., Black, P.L., Yao, X., & Dagan, S. (1999). Cell-based and animal models for hepatitis B and C viruses. Antiviral Chemistry & Chemotherapy, 10, 99-114.


 March 27th is
March 27th is  Around the world, the most common mode of hepatitis B transmission is from mother to child. Unfortunately, pregnant mothers who have hepatitis B can transmit the virus to their newborn during the delivery process. 90% of these HBV infected babies will progress to chronic infection putting them at increased risk of serious liver disease or liver cancer later in life.
Around the world, the most common mode of hepatitis B transmission is from mother to child. Unfortunately, pregnant mothers who have hepatitis B can transmit the virus to their newborn during the delivery process. 90% of these HBV infected babies will progress to chronic infection putting them at increased risk of serious liver disease or liver cancer later in life.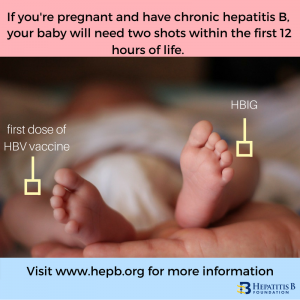 The
The  Around the world, millions of people with chronic hepatitis B face wrenching discrimination that limits their dreams, education, careers, income and personal relationships.
Around the world, millions of people with chronic hepatitis B face wrenching discrimination that limits their dreams, education, careers, income and personal relationships.

 Have you been thinking about adoption for a long time or have been inspired by NBC’s show, This is Us, to adopt? Adoption is exciting! However, it can be nerve wracking and feel overwhelming. We at the Hepatitis B Foundation can help with one aspect of the adoption process – making sure you have accurate information about hepatitis B.
Have you been thinking about adoption for a long time or have been inspired by NBC’s show, This is Us, to adopt? Adoption is exciting! However, it can be nerve wracking and feel overwhelming. We at the Hepatitis B Foundation can help with one aspect of the adoption process – making sure you have accurate information about hepatitis B.