The tricky part about hepatitis B symptoms is that there are often no symptoms. That is why hepatitis B is referred to as a “silent infection”. This can be a little confusing to people newly diagnosed with HBV – whether it is determined you have an acute or chronic infection.
The tricky part about hepatitis B symptoms is that there are often no symptoms. That is why hepatitis B is referred to as a “silent infection”. This can be a little confusing to people newly diagnosed with HBV – whether it is determined you have an acute or chronic infection.
If you have a new, acute infection, there is a good chance you will be one of the roughly 69% with no notable symptoms. You may feel a little under-the-weather or a little more tired then usual, or you may notice no difference at all. You may learn about your infection through blood work following a possible exposure, or following screening from a blood donation. Since 90% of adults infected with hepatitis B will clear the infection – most with no medical intervention, it is possible for you to be infected, clear the virus, and never even know until blood work shows evidence of a past infection.
Then again you may be one of the roughly 30% who do have symptoms. You may experience flu-like symptoms such as achy muscles and joints, a low-grade fever and fatigue. Because your liver plays a role in digestion, you may experience a loss of appetite, feel a little nauseous, or experience pain in the upper right quadrant of your abdomen. You may have dark, tea colored urine. Then again, these symptoms may not be so severe that you take much notice. It’s okay, because these symptoms typically do not require treatment. However, if you are symptomatic, or you are concerned, please see your doctor, so blood tests can be run to be sure your liver is safe.
Here are the important symptoms that you need to have checked-out immediately: jaundice, severe nausea and vomiting, and bloating or swelling of the abdomen. If you have any of these symptoms, you need to seek immediate medical attention. Your doctor will want to run blood work, which will likely need to be repeated while you are symptomatic and as you recover, to monitor your condition and be sure you are safe. At this time, your doctor will determine the next steps –perhaps you will need to be admitted to the hospital for fluids and observation if you are severely dehydrated, or more likely, you’ll recover at home with regular lab work and follow-up with your doctor.
If you notice that your skin or the whites of your eyes are yellow, then you are suffering from jaundice. This is due to a build-up of bilirubin in the blood and tissues. Your liver is an amazing organ and one of its responsibilities is the filtering out of your body’s bi-products or other toxins from your blood, maintaining them at healthy levels. Jaundice is very unsettling to those that have it because it is noticeable by others. Normal coloring will return once the body is able to rid itself of the buildup of these toxins.
Although rare, (approximately 1%) acute hepatitis B can result in life-threatening, fulminant hepatitis, which can lead to liver failure. Fulminant hepatitis requires immediate medical attention.
The other possibility is that you are actually chronically infected, and that your infection is not new, or acute. You may have been living with HBV since birth or early childhood. Your hepatitis B infection may be a complete surprise to you. You might ask, “How could I have this infection all of these years and not even know it?” Once again, HBV is a silent infection. For those chronically infected, obvious symptoms may not occur for decades. The liver is a hard-working, non-complaining organ, but you don’t want to ignore your HBV and put yourself at increased risk for cirrhosis, liver failure or liver cancer. Believe it or not, the sooner you learn about your HBV infection, the better, so that you get regular monitoring, seek treatment if necessary, and make lifestyle changes that are good for your liver and overall health.
Whether you have symptoms or not, there are a few things you need to remember. You must go back to your doctor for further lab work to determine if your HBV infection is acute or chronic. If you are still surface antigen positive (HBsAg+) after 6 months, then you have a chronic infection and need to see a liver specialist to learn more about your hepatitis B infection. The other thing you must do is take precautions so you do not transmit hepatitis B to sexual partners and close household contacts. Fortunately, HBV is a vaccine preventable disease. Finally, be sure to take care of your liver by eating a well-balanced diet, avoiding alcohol, and talk to your doctor or pharmacist about prescriptions or OTC drugs that may be hard on your liver.






 The annual Hep B United Summit, organized by the
The annual Hep B United Summit, organized by the 




 The news was all good. His children had been immunized and were fine, he was not infected and was immediately immunized. Today, we are all doing fine, including our daughter.
The news was all good. His children had been immunized and were fine, he was not infected and was immediately immunized. Today, we are all doing fine, including our daughter.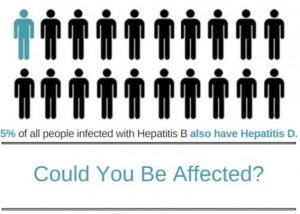 By Christine Kukka
By Christine Kukka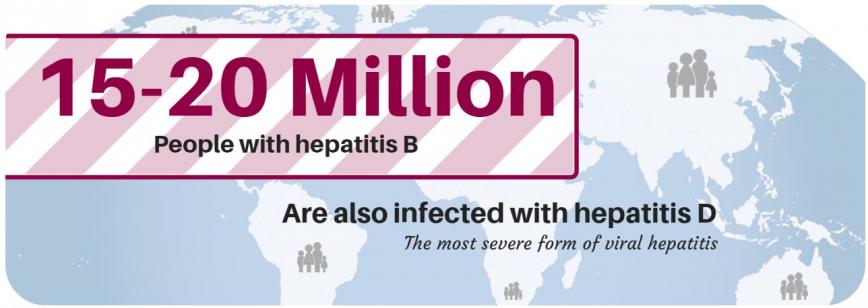 What medical conditions suggest hepatitis D? Anyone with chronic hepatitis B who is not responding to antiviral treatment, or who has signs of liver damage even though they have a low viral load (HBV DNA below 2,000 IU/mL) should be tested. Fatty liver disease (caused by obesity) and liver damage from alcohol or environmental toxins should be ruled out before testing for hepatitis D.
What medical conditions suggest hepatitis D? Anyone with chronic hepatitis B who is not responding to antiviral treatment, or who has signs of liver damage even though they have a low viral load (HBV DNA below 2,000 IU/mL) should be tested. Fatty liver disease (caused by obesity) and liver damage from alcohol or environmental toxins should be ruled out before testing for hepatitis D.