William and his family. Click here to watch his story.
By Christine Kukka
After our daughter was diagnosed with chronic hepatitis B 20 years ago, my doctor explained that every household member, including my husband, had to be tested for the liver infection that’s transmitted by direct contact with blood and body fluids. ASAP.
The good news was my daughter was healthy and had no signs of liver damage, but my husband and I were shaken to the core by her diagnosis. Weighed down by worry and ignorance, I feared we might all be infected and faced a death sentence.
I drove out to my husband’s work and we went for a walk. I explained what the doctor had said and explained he had to get tested. It was one of those moments when fear and denial play out over the course of a conversation. Like everyone, he was afraid to get tested. He felt fine, at first he didn’t want to know whether he was infected. For a few moments, he thought ignorance might be less painful than finding out he had hepatitis B.
And, as in most families, this disclosure wasn’t easy. He had children from his first marriage who were with us every weekend and they had to be tested too. He would have to share this information with his former wife. This disclosure was going to upend two households. After a few minutes of waffling and processing, he did what courageous fathers do. He got tested and made sure his children were tested too.
The news was all good. His children had been immunized and were fine, he was not infected and was immediately immunized. Today, we are all doing fine, including our daughter.
Every father’s day, I think about that moment, when my husband refused to retreat into denial, and put his family’s health ahead of his initial impulse to hide from a frightening and messy situation. It is what being a good father is all about, and it takes courage.
For another story about hepatitis B and fatherhood, please view the Storyteller video featuring William’s Story: #justB Dad by clicking here.
Excited by the impending birth of his first child, William decided to plan for his family’s financial future. He was shocked to learn through a required health insurance blood test that he had hepatitis B. He spent sleepless nights wondering how he contracted the virus and whether it was a death sentence. After wading through dense layers of information online, he went in for more tests and was reassured by a caring provider that with monitoring, dietary changes and an active lifestyle, he would live a long life.
He realized that knowing where hepatitis B came from isn’t as important as focusing on staying healthy.
The CDC offers short video clips that feature a conversation between a daughter and her parents, with the daughter explaining why Asian-Americans should be tested for hepatitis B in English, Cantonese, Mandarin, Vietnamese and Korean. A high percentage of Asian and African immigrants have hepatitis B, but most don’t know they are infected. To view these clips, visit: http://www.cdc.gov/knowhepatitisb/materials.htm
Join Hep B United, the National Viral Hepatitis Roundtable, NASTAD and CDC’s Division of Viral Hepatitis for a Twitter #HepChat at 2 p.m. (EST) Thursday, June 8. The chat will highlight Hepatitis Awareness Month outreach events and allow hepatitis B and C partner organizations to share their successes, challenges and lessons learned from their efforts.
By Joan Block, RN, BSN, Executive Director and Co-Founder
The story of the Hepatitis B Foundation is a love story that’s never been told. In June, I will retire after 25 years of service, so now feels like the right time to share my personal story.
In 1987, I was diagnosed with hepatitis B. I had just married Tim (co-founder and president of the foundation and its research affiliate, the Baruch S. Blumberg Institute) when my doctor suggested I get tested for hepatitis B because I was born in Korea.
We were devastated by the diagnosis. As a young nurse in the 1980s, the only hepatitis B patients I knew were dying of liver failure or liver cancer. They were kept in isolation rooms where I had to wear a gown, gloves, and mask to even provide them with basic care.
This was a dark and scary time for us. There was nowhere to turn for information or support, and no available treatment. The prospect of our life together was overshadowed by fear and uncertainty.
My husband Tim, a research scientist, took immediate action by changing his focus to hepatitis B and began the quest to find a cure. We reached out to our close friends, Paul and Jan Witte, and together we decided to create a nonprofit organization dedicated to finding a cure for hepatitis B and helping those affected.
In 1991, the Hepatitis B Foundation was officially established. A quarter of a century later, the foundation has grown from a grassroots effort into the world’s leading nonprofit research and disease advocacy organization solely dedicated to hepatitis B.
Joan M. Block, RN, BSN, Co-Founder and Executive Director
There are many reasons why I waited so long to share my personal story. At first, it was fear and shame. The stigma of having an infectious disease was strong, even though I had acquired hepatitis B at birth. Later, I wanted to keep the focus on the mission of the foundation, not on my personal story.
Today, however, I realize that there is a compelling need for people like myself to publicly share their stories. We need to break the silence around hepatitis B. Personal stories are a powerful tool to increase awareness, decrease stigma and end discrimination.
Although I am stepping down as executive director, I will continue to be passionately involved in advancing the foundation’s mission to find a cure. I will also use every opportunity to personally give voice to the more than 257 million people affected by hepatitis B worldwide.
If more of us can stand up and say without fear or hesitation, “I have hepatitis B,” then we will indeed contribute significantly to making hepatitis B history!
Thank you.
In recognition of Joan’s dedicated service, the Board of Directors has created the Joan Block Improving Lives Fund of the Hepatitis B Foundation. This fund will enable the foundation to advocate powerfully to increase research funds for a cure, end discrimination against those affected, and increase screening, prevention and care to save more lives from hepatitis B.
To honor Joan’s valuable legacy, please make a donation at our secure website by clicking here.
Image courtesy of David Castillo Dominici at FreeDigitalPhotos.net.
By Christine Kukka
Don’t know your hepatitis B status? Get tested. Worldwide an estimated 90 percent of people with chronic hepatitis B don’t know they’re infected. In the U.S. only 25% are aware of their infection. Unfortunately, many doctors won’t test you for hepatitis B unless you request the test. If you or your parents come from or live in a country with high rates of hepatitis B, or if you’ve been sexually active or have other risk factors , get tested. It could save your life.
Get tested for sexually-transmitted infections (STIs). More than half of us will have an STI in our lifetime, and in the U.S. about half of new hepatitis B infections are sexually-transmitted. Many doctors don’t test for STIs. In a national survey of U.S. physicians, fewer than one-third routinely screened patients for STIs. To make matters worse, many women are afraid to talk to doctors about their sexual history and STI risk. Be brave, ask your doctor to test you for STIs and hepatitis B if you think you are at risk.
Photo by Amanda Mills of CDC.
Get immunized against hepatitis B. Not sure if you’ve been immunized during childhood? Tell your healthcare provider and get tested and immunized. Even if you were vaccinated in the past, getting a second vaccine series won’t harm you. If your partner has hepatitis B, getting vaccinated is critical to protect your health. Get tested first. Practice safe sex until you have received all three shots. About one to two months after your third shot, get tested for the hepatitis B surface antibody (called titers). If you have at least 10 mIU/mL of surface antibodies, you are permanently protected against this serious liver disease.
Infected? In Love? Disclose. When you disclose your hepatitis B status before sex – even if it’s safe sex with a condom – you don’t jeopardize your partner’s health or his/her trust in you. Talking about hepatitis B helps reduce the stigma surrounding this infection and may prompt the person to get vaccinated. How do you tell a potential partner that you have hepatitis B? Calmly and carefully. Do some research so you have a thorough understanding about hepatitis B, which will make it easier for you to calmly explain it. The more you know, the less you fear, and the more comfortable you will be in dispelling their fears and conveying a sense of truth and integrity.
Insist on sterile medical and tattoo equipment. Hepatitis B can live for several days on hard surfaces, including improperly-sterilized and re-used syringes and other medical devices. Whether you’re going for a tattoo or to a dentist or doctor’s office, it is your right to insist that all equipment is brand new (ask to see it removed from protective packaging) and properly sterilized. Visit a licensed, professional tattoo parlor and make sure all tattoo equipment has been sterilized and that needles come out of new packages.
Image courtesy of patrisyu at FreeDigitalPhotos.net
Infected and pregnant? Protect your baby from hepatitis B.
Make sure your newborn gets the hepatitis B vaccine within 12 hours of birth. Nearly all hepatitis B-infected women will pass the infection onto their children during delivery, but you can stop that infection cycle. In about 90 percent of cases, immediate immunization will prevent infection. In some countries, it may be difficult to get just the single hepatitis B vaccine dose, but if you are able to immunize your baby at birth, you will have protected your child against a potentially dangerous liver disease. If you live in an area where HBIG (hepatitis B antibodies) is available, make sure your newborn is also given a dose of HBIG at birth, this adds another layer of protection against infection.
Get your viral load (HBV DNA) tested early in your pregnancy. Some women with high viral loads (exceeding 200,000 IU/mL or 1 million copies/mL) are at high risk of infecting their newborns, even if the baby receives the first vaccine dose within 12 hours of birth. Ask your doctor to test your viral load, if it’s high, medical guidelines recommend treatment with the antiviral tenofovir during the last three months of your pregnancy to lower your viral load. If you doctor doesn’t test your viral load, be assertive and ask for the test, especially if you are HBeAg positive.
Breastfeeding is OK, even if you have hepatitis B. If you’re infected with hepatitis B, you can safely breastfeed your baby, as long as the baby was vaccinated against hepatitis B at birth.
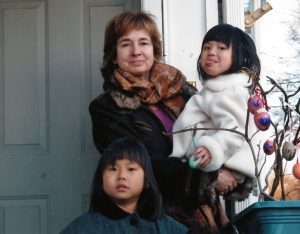
Maureen and her two daughters
Your children infected? Don’t wait to start talking to them about hepatitis B. You need to start talking to them about germs and how to keep themselves and others safe when they’re young. (Listen to Jin’s Story #justB You about growing up with hepatitis B.) This conversation will be one of the hardest discussions you will ever have with your child, and you’ll be talking about it often in the years ahead, but you can do it! Start explaining HBV by reading the Hepatitis Victoria “Hep B Hero” book for children two to six years of age.
To hear how other mothers handled talking about hepatitis B with their children, visit our Storytelling page and click on Maureen’s Story #justB Brave and Maureen K’s Story #just B Assertive to hear how these mothers navigated issues of disclosure and stigma with their daughters. Hepatitis Victoria recently launched their “Little Hep B Hero” book, an engaging story teaching children 6-12 year olds about hepatitis B.
Talk to your children about sex and safe sex practices. It’s critical to educate young people about sexual health and STIs. If we want our sons and daughters to feel empowered to take care of their sexual health, we have to change the culture that dictates the way we talk – or don’t talk – about sex. That means removing denial, uncertainty and shame so we have better conversations about sexual health, sexual assault prevention and STIs. It’s also important to encourage our children to have frank sexual health discussions with one another.
Take care of your health, get monitored regularly: It is important to get your hepatitis B monitored regularly – at least every year and more often if you have liver damage. Women living with hepatitis B tend to have lower rates of liver damage than men because estrogen appears to help protect the liver. But even if we lead a healthy lifestyle and avoid alcohol and cigarettes, as we age our immune system weakens and our viral load (HBV DNA) can start to rise. There is no cure yet for hepatitis B, but there are effective drugs that lower viral load and reduce the risk of liver damage.
Renseley and her husband.
Be happy. A mother or woman who is well rested, enjoys a healthy diet, gets plenty of exercise, has good relationships with friends and family members and knows how to ask for help when she needs it, is far better equipped to be happy and be the best mother she can be. It isn’t selfish to take care of yourself. Tough times happen, and sometimes a friend or family member may need us, and we will need to be strong during difficult times. If we take care of ourselves and ask for help, in the long run happiness will prevail. For a profile in joy and courage while fighting hepatitis B in her family, watch Renseley’s Story #justB Strong.
The Hepatitis B Foundation is proud to launch its storytelling campaign, sharing the stories of people living with and affected by hepatitis B. Join the Twitter interview at 2 p.m. (EST), Tuesday, May 16, hosted by the Hepatitis B Foundation and StoryCenter.
We will introduce three of our storytellers and their stories. Join the Twitter interview with the hashtag #justB and hear the poignant stories of real people living with hep B.
We will be introducing Jason, Bunmi and Maureen K. Jason, was in a difficult place in his life with addiction and depression when he learned of his hepatitis B and sought treatment. Bunmi, originally from Nigeria, talks about the loss of her father to hepatitis B- related liver cancer and the unwillingness of her family to talk about his disease. Maureen’s hepatitis B journey began with the adoption of her daughter, and the struggle with disclosure with family and friends. These brave storytellers are ready to put an end to the silence surrounding hepatitis B.
Below are the topics scheduled for discussion during the Twitter interview. How can you contribute to the conversation? Please support Jason, Bunmi and Maureen K. as they disclose their hepatitis B stories on social media. Consider sharing parts of your hep B story or pose a question. Join the conversation with the hashtag #justB.
T1. Tell us about hepatitis B, the storytelling campaign and what the foundation hopes to achieve for those affected by hepatitis B.
T2. What makes hepatitis B different from other diseases, and how do these stories highlight the challenges associated with hepatitis B?
T3. We’d like to open it up to our storytellers. Please tell us about your story, and what makes hepatitis B different from other diseases.
T4. How has hepatitis B affected your life?
T5. What made you decide to share your hepatitis B story? Were you concerned with the stigma associated with hepatitis B?
T6. Describe your experience meeting with others impacted by hepatitis B.
T7. If there is one message you would like to get across to others about coping with #hepatitis B, what would it be?
T8: What would you tell others that are struggling with whether or not they should share their hepatitis B story?
Are you just getting started with Twitter and want to know how to join the conversation? Type #justBin the search box of the Twitter application and click on the “latest option” to follow the twitter view.
You can prepare any questions or tweets you might have for the above participants in advance, or you can also tweet on the fly, re-tweet, or Like a tweet from the chat.
The topics are labeled T1, T2, etc. so please respond/answer specific topic by using A1, A2, etc. in front of your tweets. Remember to include the #justBhashtag, which is not case sensitive, in all of your tweets.
Looking forward to sharing the stories of our guests on the Twitter view. Please welcome them by joining the conversation!
Alan Wang of Berkeley, CA, describes how doctors failed to test his family for hepatitis B in his video story.
In an innovative storytelling initiative, people living with chronic hepatitis B open their hearts and share their stories of family secrets, stigma and diagnoses that came too late as they confront the impact of hepatitis B on themselves and the people they love.
The Hepatitis B Foundation, working with StoryCenter, has created unique video stories that share the experiences of people affected by hepatitis B, which affects one-third of the world’s population. The video stories, which debut May 1 in recognition of Hepatitis Awareness Month, are designed to raise awareness about the liver disease that affects 2 million in the U.S.
There is no better way to understand the human toll hepatitis B takes than to hear directly from those affected. Most people know very little about this disease and up to 75 percent of people living with hepatitis B don’t know they’re infected. The hope is that these stories will put a human face on this infection and help improve testing, vaccination and treatment.
One storytelling video, featuring former ABC 7 News anchor Alan Wang of Berkeley, CA, talks about how doctors fail to test people for hepatitis B. It was after the CEO of Newsworthy Media suffered liver damage that a doctor tested him for hepatitis B. “It was only because I (had) a medical reporter friend who connected me to a leading hepatologist that I got the attention I needed,” Wang, 49, explains in his story. After his diagnosis, he encouraged family members to be tested and his mother and siblings were also found to be infected by the disease that is easily transmitted at birth.
“We were left to connect the dots because the medical profession is failing to address an epidemic that kills more than 700,000 people a year,” he explained. “It’s bad enough that hepatitis B is a silent killer with few symptoms until it’s too late. It’s also ignored by Asian cultures that consider talk about deadly diseases to be taboo.”
While a safe and effective vaccine that prevents hepatitis B has been available since 1982, many Americans did not have access to the vaccine. John Ellis Jr., another hepatitis B storyteller who lives in Pensacola, FL, was diagnosed with chronic hepatitis B at age 16. He, like many people living with hepatitis B, does not know how he became infected.
“When I was first diagnosed, I was shocked the doctor couldn’t tell me how I contracted it, as if finding out how I contracted hepatitis B would somehow cure me of it. As I grow older, what’s most important to me is maintaining my health.” Ellis explains in his story that he wants to be, “bigger than his diagnosis.” He does not want hepatitis to hold him back or define him. He is an entrepreneur and he has organized a charity bike ride to raise awareness and funding for research.
Another featured storyteller is pharmacist Bunmi Daramaja, of Elkridge, MD, who grew up in Nigeria and emigrated to the U.S. She struggled with her family’s reluctance to discuss her father’s death from liver cancer, resulting from chronic hepatitis B.
“Stigma is everywhere (in my African culture),” she explained in her story. “People don’t think about the facts of how the virus is transmitted– they are afraid to even touch someone who has it. Many people don’t even want to get tested, because treatment is either not available or costs too much money. They say, ‘What’s the point?’ This needs to change.
“In the U.S., the services are here, and I want to make sure that people of African origin know there are resources. I want to end this silence,” she explained.
The Hepatitis B Foundation’s Storytelling page helps tell the story about an infection in the U.S. that is under-diagnosed, under-treated and remains stigmatized across America.
When my daughter thinks about how active she should be in raising awareness about hepatitis B, she gets tripped up by racial identity and politics.
Recently, she attended a workshop where people living with hepatitis B told their stories. It was empowering and energizing, and then she went home to a state where the majority are white, the governor claims immigrants are bringing in new diseases, and no one has ever heard about hepatitis B.
“Suddenly, I feel paralyzed,” she told me. “I look at the other people in my hepatitis B group and all of us were Asian or Black. I’m afraid if I tell my story here at home that everyone will assume everyone who’s Asian has hepatitis B.”
Instead of increasing white America’s compassion and empathy towards people with hepatitis B, she fears it might make them more afraid of people of color. Her fears are understandable. In this era of Trump, hate crimes and backlash against immigrants have increased. She’s afraid speaking out might unwittingly reinforce simmering racist stereotypes. She wonders if she has that much courage.
She’s worried about how it will affect her personally. Already she sees some clients she works with gravitate and open up more to her white coworkers. “I don’t know if I’m over-thinking it all, and feeling overwhelmed about how to handle this,” she confided.
There is a story about a Asian-American researcher who worked on hepatitis B for decades. When she conducted some independent screening in her community and discovered that a large percentage of Korean-Americans tested positive for hepatitis B, she was fearful. She never published her findings, she was afraid it would fuel racism against Asian-American immigrants. She chose self-censorship instead.
Much has been written lately about how much more empathy the American public and some politicians appear to have toward the rural opiate addiction crisis now that it has a “white face,” given that addiction in inner cities has decimated generations of African-Americans for decades.
Does my daughter intuitively know that America has far more sympathy (and dedicates more funding) for diseases that affect white and middle-class communities than minority populations?
I try to give her another take on the situation, suggesting that the human map of hepatitis B is defined by access to healthcare. People in poor regions of the world don’t have access to the hepatitis B vaccine birth dose, which must be administered within 12 hours of birth to break the mother-to-child infection cycle, or to sterile syringes and medical equipment.
I explain it’s the same in rural America. The hepatitis B vaccine has been available since 1982 and recommended for all children and adolescents, yet today there is an uptick in new hepatitis B infections among injecting drug users. Uninsured adults who didn’t have access to preventive healthcare and the hepatitis B vaccine growing up are now getting infected from the opioid epidemic. Just like Africa and Asia, medical insurance and access to healthcare defines who lives and dies.
Just like Africa and Asia, in rural and low-income America, access to insurance and healthcare defines who lives and dies.
In the late 1980s, a young group of AIDS activists created ACT Up, a noisy, boisterous group that fought the government and big pharma in order to speed up the AIDS drug approval process. They even took over the National Institutes of Health office at one point and unfurled a banner that read: Silence = Death.
For a long time, white America thought everyone who was gay had AIDS. But over time, they stopped making that assumption. It takes time, education, and tireless and selfless advocacy. We all do what we can, when we can.
I am a retiree and volunteer working to address hepatitis B discrimination, which involves a serious, relatively unknown chronic disease that impacts Asian-American and Pacific Islander American (AAPIA) immigrants and refugees who are often isolated by culture and language, which makes this discrimination especially egregious.
As a fifth-generation AAPIA, I’d heard of hepatitis B but was not aware that it leads to cirrhosis or liver cancer or that AAPIAs make up 50 percent of the country’s estimated 2 million hepatitis B cases, but represent less than 5 percent of the U.S. population.
These facts came into sharp focus in 2010, when a college senior was devastated to learn she would not be permitted to enroll in a healthcare program due to her chronic hepatitis B. Nothing in the school’s admissions policy or information published by the profession’s national admissions coordinating agency had prepared the student for this. When the student informed me that an older friend with hepatitis B was completing a similar healthcare program at a different institution, I advised her to challenge her school’s exclusion policy.
The issue raised many questions that called for research and consultation with hepatitis B specialists and community health and civil rights advocates to find out how and why schools were permitted to have such different hepatitis B policies. I also sought to compare various institutional policies with their respective state licensing laws for providers with hepatitis B. Fortunately, I was referred to an attorney who had an understanding of the disease who challenged the school’s exclusion policy. This led to the school’s implementation of a new, progressive policy for students with chronic hepatitis B.
Though gratified with the outcome for this student, I feared other students with hepatitis B would face similar discrimination, because too many medical school policies barring enrollment of students with hepatitis B were undisclosed. Future victims might not know how or where to access assistance or legal help. Given the World Health Organization’s map of global regions with high rates of hepatitis B and the current patterns of U.S. immigration, I believed hepatitis B discrimination would soon impact other immigrant/refugee communities.
My initial contact with the Hepatitis B Foundation in 2010 developed into a working relationship that won justice for five additional medical and dental students who contacted us between 2011 and 2013.
At the urging of the foundation and hepatitis B specialists, the Centers for Disease Control and Prevention (CDC) revised and updated its 20-year old policy for infected healthcare workers; and the disability complaint I filed with the Department of Justice (DOJ) resulted in a Settlement Agreement for two students and a Technical Assistance Letter jointly issued by three federal agencies to inform healthcare schools of their responsibilities to accommodate individuals with hepatitis B and point out that failure to comply could also violate Title VI, which prohibits discrimination on the basis of race, ethnicity or national origin.
Hepatitis B civil rights advocacy is now focused on policies of all U.S. military services, including the Coast Guard, Public Health Service and the National Oceanic and Atmospheric Administration, which ban individuals with hepatitis B from joining.
Between 2013 and 2016, we advised nine active duty personnel and students who were not permitted to enlist for military service or scholarship programs or were discharged from active duty or a U.S. military academy due to hepatitis B. We continue to advocate for the Department of Defense to revise the policies that prohibit the people with chronic hepatitis B and establish reasonable, science-based accommodation policies for existing or future personnel who are diagnosed with chronic hepatitis B
Continuing hepatitis B education and civil rights challenges
Most immigrants and refugees do not understand the seriousness of the silent disease or the importance of hepatitis B screening. If diagnosed with hepatitis B, they often fear being treated as ‘pariahs’ in a society where they already feel like outsiders; or they worry that others in their family will be stigmatized or that hepatitis B will be used as an excuse to prevent immigrants from entering the U.S. Still others may be silenced by a code of silence within their professions.
Adding complexity to hepatitis B education and outreach are the diverse languages and cultures of the immigrant/refugee communities, along with the economic and social disparities experienced by so many families who start new lives in the U.S. living in relative isolation with limited English proficiency and few financial resources.
Lest we think hepatitis B discrimination is limited to Asian- and African-American and immigrant/refugee communities, new pockets of hepatitis B infection linked to the opioid epidemic have been reported in rural regions. Outbreaks of hepatitis B infection in majority white, non-immigrant, economically-depressed regions suggest that some of those infected may not have been immunized due to a lack of knowledge or healthcare access. These are social and economic disparities that mirror the disparities experienced by many immigrant/refugee families.
Like their healthier peers, teens and young adults with hepatitis B seek opportunities to fulfill their potential, earn a living wage and improve their lives. To this end, hepatitis B advocates are working to protect the rights of infected persons and ensure that our schools and institutions, and public and private employers administer reasonable, science-based chronic hepatitis B policies and accommodations.
Nadine Shiroma is a community civil and voting rights advocate and policy advisor to the Hepatitis B Foundation. She can be contacted at nadine.shiroma@gmail.com.
Diagnosed in March, 2009, with stage 4 metastatic non-Hodgkin’s lymphoma, Nadine spent the remainder of the year undergoing chemotherapy and recurrent hospitalizations. “That I lived and recovered is due to doctors at the City of Hope Cancer Research Center, my family and especially my husband and daughter,” she recalled. “Assisting the college senior in 2010 helped me discover a new normalcy. On that day in 2011, when a new, progressive chronic hepatitis B accommodation policy was published by the healthcare school that previously excluded students with hepatitis B, I told myself, ‘This is why I lived.’”
Image courtesy of vectorolie at FreeDigitalPhotos.net.
By Christine Kukka
One of the most glaring civil rights abuses facing people with hepatitis B in the United States today is the military’s continued refusal to allow anyone with chronic hepatitis B to enlist.
This prohibition continues, despite the fact that all military personnel are vaccinated against hepatitis B, and scientific data shows hepatitis B is not spread through casual contact.
“Our brave servicemen and women deserve nothing less than the best, yet many qualified individuals are being prevented from serving in specific roles and/or being promoted within the military’s ranks. That’s simply wrong,” said U.S. Rep. Barbara Lee, D-Calif., in a letter challenging the military’s Uniform Code of Military Justice prohibits people with hepatitis B and C and HIV from enlisting in the Navy, Army, Air Force, Coast Guard, Marine Corps and National Oceanic and Atmospheric Administration.
This outdated and scientifically-baseless Department of Defense policy damages the civil liberties of many Americans.
Asian and Pacific Islander Americans, African and Middle Eastern immigrants and other ethnic groups are disproportionately impacted by hepatitis B. For example, Asian-Americans make up less than 5 percent of the total U.S. population but account for more than 50 percent of the 2 million people living with hepatitis B cases in the U.S.
Immigrants and their children are also disproportionately affected by hepatitis B, due to the lack of vaccinations in their countries of origin. As a result, they are barred from military service, which offers a path to citizenship.
What is especially heart-breaking are the young men and women who work hard to get into prestigious military academies, only to be dismissed when it’s discovered they have hepatitis B.
This military code historically barred people with serious medical conditions because they were considered unfit to serve, suspected to incur high healthcare costs and could pose an infection risk to fellow soldiers.
The code prohibits enlistees with the, “Presence of … current acute or chronic hepatitis carrier state, hepatitis in the preceding six months or persistence of symptoms after six months, or objective evidence of impairment of liver function.”
But most people with chronic hepatitis B who want to enlist are healthy, have no liver damage, do not pose an infection risk to others, and are capable of performing the same duties required of their fellow recruits. Clearly, military policy has not caught up with current science.
This discriminatory policy is difficult to challenge, despite the best efforts of advocates including Rep. Lee and U.S. Rep. Ileana Ros-Lehtinen (R–FL).
The Americans with Disabilities Act, which prohibits discrimination against people with disabilities and chronic diseases such as HIV and hepatitis B and C, unfortunately has no jurisdiction over the Department of Defense.
Although the Department of Justice and CDC have issued clear, science-based guidelines that find hepatitis B-infected healthcare providers to pose no infection threat to patients or coworkers, the military continues to practice its discriminatory policies, which rob the military of talented and motivated recruits.
It is time to change these outdated and discriminatory policies. There are many good men and women waiting, willing and able.
Image courtesy of Janpen04081986 at FreeDigitalPhotos.net.
By Christine Kukka
The day we arrived home from China, my husband and I brought our four-month-old adopted daughter to a pediatrician for a check-up. The doctor looked at my daughter’s health records from China, saw she had tested negative for hepatitis B, and said, “Good, I don’t have to test her for that.”
About a year later, I got sick, very sick. I felt nauseous, my stomach hurt and I felt bone tired. I gradually recovered and chalked it up to a bad case of flu.
When my daughter was 2 years old, I read on an adoption email list that some children were testing positive for hepatitis B stateside, though their medical reports in China had given them a clean bill of health. During her next check-up, I asked the pediatrician to test her for hepatitis B. The test result came back positive. A week later, so did mine.
My daughter had chronic hepatitis B, and I, who had donated blood regularly until I became a busy parent, had an acute case, and cleared the infection. Our story, unfortunately, is not uncommon. Across the U.S., many primary care doctors fail to test at-risk patients for hepatitis B.
I live in a rural, New England state where there are not many people from countries with high rates of hepatitis B. Our pediatrician didn’t know that it can take several weeks after exposure for an infection to show up in a lab test. She didn’t know that China’s medical records weren’t reliable. She knows it now, but many providers still don’t.
Over the years, I have heard many similar stories with worse outcomes. In one case, a young woman born in South Korea suffered epilepsy and her doctor treated her with a common seizure medication without first screening her for liver infection or damage. She died in her early 20s from liver cancer. The epilepsy drug accelerated her hepatitis B-related liver disease.
A recent article published on the Monthly Prescribing Referencewebsite, describes how a primary care provider was sued for malpractice after he failed to monitor a patient for liver damage despite the fact the Asian-American patient told him he had hepatitis B in his teens. The patient, who was treated by the doctor for more than 15 years, died from liver cancer resulting from untreated hepatitis B.
In addition to these stories, there are numerous studies published in medical journals that show doctors often fail to test patients for hepatitis B or treat them appropriately when hepatitis B is diagnosed. Even liver experts who should know better often don’t follow medical guidelines that recommend antiviral treatment for hepatitis B-related liver damage.
I often wonder why there is this breakdown in hepatitis B care. I wonder if it stems from racism or prejudice. Many people with hepatitis B are people of color, recent immigrants, gay, or low-income. These patients can be challenging for doctors, especially when providers have little experience with hepatitis B, but that’s no excuse.
Over the years, I have accompanied my daughter to her medical appointments and often remind doctors what labs they should order and what the latest monitoring guidelines are. The best of them admit they don’t know how to treat hepatitis B and sit down and read the latest guidelines and discuss a care plan with my daughter. The worse simply do whatever I ask, and I am no doctor.
I have found one of the best tools available are software programs that link a patient’s electronic medical record to current medical guidelines. It makes it easy for doctors to know what tests should be ordered, especially if they have never treated hepatitis B before. But they need to have the software and the desire to use it.
I appreciate that doctors are human, over-worked and are driven by an assembly line business model that makes it hard to pause and research a new medical condition. However, the human price paid for lapses in care is terrible, and far more costly considering the expense of treating liver cancer, compared to running the right tests and prescribing the correct antiviral treatment today.
In the U.S., about two-thirds of people living with chronic hepatitis B don’t know they’re infected. They don’t have the money, the insurance coverage, or access to the right doctors who will test and treat them, and make sure their family members are tested and vaccinated. An estimated 20 percent of these people will die prematurely from liver disease. And today, as I listen to the news, I am afraid it’s only going to get worse.


 The news was all good. His children had been immunized and were fine, he was not infected and was immediately immunized. Today, we are all doing fine, including our daughter.
The news was all good. His children had been immunized and were fine, he was not infected and was immediately immunized. Today, we are all doing fine, including our daughter.






 The
The 

 “We were left to connect the dots because the medical profession is failing to address an epidemic that kills more than 700,000 people a year,” he explained. “It’s bad enough that hepatitis B is a silent killer with few symptoms until it’s too late. It’s also ignored by Asian cultures that consider talk about deadly diseases to be taboo.”
“We were left to connect the dots because the medical profession is failing to address an epidemic that kills more than 700,000 people a year,” he explained. “It’s bad enough that hepatitis B is a silent killer with few symptoms until it’s too late. It’s also ignored by Asian cultures that consider talk about deadly diseases to be taboo.” By Christine Kukka
By Christine Kukka

 This military code historically barred people with serious medical conditions because they were considered unfit to serve, suspected to incur high healthcare costs and could pose an infection risk to fellow soldiers.
This military code historically barred people with serious medical conditions because they were considered unfit to serve, suspected to incur high healthcare costs and could pose an infection risk to fellow soldiers.
 I have found one of the best tools available are software programs that link a patient’s electronic medical record to current medical guidelines. It makes it easy for doctors to know what tests should be ordered, especially if they have never treated hepatitis B before. But they need to have the software and the desire to use it.
I have found one of the best tools available are software programs that link a patient’s electronic medical record to current medical guidelines. It makes it easy for doctors to know what tests should be ordered, especially if they have never treated hepatitis B before. But they need to have the software and the desire to use it.