A primary goal of the Hepatitis B Foundation has always been to find a cure for the disease. When we ask Dr. Timothy Block, The Hepatitis B Foundation’s president and co-founder, about progress towards a cure by the many scientists worldwide working on that challenge, he considers many different angles.
The clinical definition of a cure Dr. Block favors is for someone who has hepatitis B to regain the liver health and low liver cancer risk enjoyed by someone without hepatitis B. That goal is considered too ambitious by most clinicians. A more realistic goal is sustained, drug-free, virological response for people living with hepatitis B. This means that a person for whom treatment has stopped has the same low (undetectable) viral load as when they were actively being treated on drug therapy. This already happens in a small percentage of patients and is associated with an improved clinical outcome: much less likelihood of developing serious liver disease, including liver cancer.
There is a new wave of drugs being evaluated now that Dr. Block believes may provide a sustained virological response, possibly when used in combinations with the current “standard of care”. Promising examples are what’s known as capsid inhibitors, siRNAs, NAPs/STOPs and entry inhibitors. There are even modifications of the polymerase inhibitors that have potential. As you can see in our Drug Watch page, at least 40 new treatments are now in clinical trial.
The reason it has been so difficult to find a cure for hepatitis B, Dr. Block explained, is that the virus has been around for hundreds of thousands of years and has established a mechanism to coexist with its host in a way that avoids a person’s immune system. It burrows its DNA into the nucleus of cells and is incredibly difficult to attack in ways that don’t harm the patient.
Another reason progress toward a cure has been slow, Dr. Block says, is that people with hepatitis B are simply too polite. Without a grassroots movement, hepatitis B will never get the attention and funding that other similar diseases have received.
“The hepatitis B community of scientists and stakeholders is incredibly innovative and collaborative, but we are small and underfunded,” he says. “We have made great progress in the 30 years since we started the Foundation, but that’s with a fraction of what has been spent on other diseases.”
With development of the effective COVID-19 vaccines, over the past year, we have all seen what can be done when the scientific community and governments rally around a public health crisis. “This shows that, with the right amount of money and focus, we can find a cure faster,” Dr. Block said.
“So, please, don’t be ashamed or scared of your hepatitis B diagnosis,” he added. “Seek treatment, take good care of yourself, and spread the word. Hepatitis B can be eliminated in our lifetime – we just need the support.”
It’s National Family History Day on November 25th! Today is the perfect time to sit down and talk to your family about health; it gives your loved ones an opportunity to provide the gift of a healthy future! As hepatitis B rarely has any symptoms, many people do not discover that they are infected until a family member is diagnosed or they develop liver damage or liver cancer.
Approaching the topic and starting the conversation can help to break this cycle of transmission within families and allow your loved ones to protect themselves. If you need some tips on how to start the discussion on family health, you can check out our blog post here!
Your family’s health history tells a powerful story. It guides us on what behaviors to avoid and actions that we can take to prevent developing certain illnesses or diseases. It can also help inform us on how to best navigate the health system. Do I need to be tested for liver cancer? Is the medication that I’m taking actually dangerous to my health?
When a family member is living with or has lived with hepatitis B, family health history can become even more critical to creating a healthy future. Hepatitis B is one of the world’s leading causes of liver cancer, so it is extremely important to be aware of your risk! Although hepatitis B is not genetic or hereditary – it is only spread through direct contact with infected blood or through sexual contact – multiple family members can be infected without knowing. This is because hepatitis B often does not have any symptoms and can be spread from mother to child during childbirth or by sharing sharp objects such as razors, toothbrushes, or body jewelry that may contain small amounts of infected blood. Knowing about a family members’ current or past infection is a signal to get tested for hepatitis B using the 3-panel hepatitis B blood test (HBsAg, HBsAb, HBcAb). Testing is the only way to be sure of your hepatitis B status. The test will let you know if you have a current infection, have recovered for a past infection, or need to be vaccinated.
Why does this matter if myself or a family member has recovered from a past infection?
If someone has recovered from a past infection (either acute or chronic), this is great news! Loss of the hepatitis B surface antigen may be exciting, but it does not mean that you don’t need to proceed with caution! Recovery from a past infection means that while the virus is no longer in your blood, it is still living in the liver in an inactive state. You cannot infect anyone else at this stage, but family members, and sexual partners should still get tested for the 3-panel hepatitis B blood test (HBsAg, anti-HBc, anti-HBs) because they may have been exposed in the past. Check out this helpful fact sheet on what it means to have recovered from an acute or chronic infection!
A past infection should be a part of all medical records as well. Various medications and treatments for other conditions, such as cancer or Rheumatoid arthritis have the potential to reactivate the virus that is sleeping in your liver. Some medications can suppress the immune system, which gives hepatitis B a chance to reawaken and attack the liver. Healthcare providers need to be aware if you had a past infection so that they can monitor you and potentially prescribe medications to prevent the virus from reactivating in your body.
Not every treatment will cause hepatitis B to reactivate, so it is important to be aware of the ones that carry a risk! Any treatment that suppresses the immune system such as chemotherapy and other cancer therapies, and certain arthritis, Crohn’s disease, Ulcerative colitis, asthma, and psoriasis drugs may pose a risk of hepatitis B reactivation. You can find a list of specific drug names and their risk levels on our website, but you should always consult your doctor or provider for the most accurate information.
Every medication also comes with a warning label that you should read carefully. This section will let you know if there is a risk of reactivation. You can also use the National Institute of Health’s LiverTox website to search the name of the treatment and see if there is a risk!
Talking to Your Family
Hepatitis B may increase a person’s risk of liver disease and liver cancer but with knowledge of an infection, you can take measures to help manage it. For family members who have not been infected, they can take action to prevent future infection by getting vaccinated! Many people assume that they have already been vaccinated, but this is not always the case. Globally, adult completion rates of all 3 doses of the vaccine are low, meaning that most adults are vulnerable to infection. The vaccine is highly effective and is the best form of protection against the virus. Don’t assume you have been vaccinated; check your immunization records or ask your doctor!
Spending your holiday talking about health may not sound like fun, but it is extremely important – it may even change your life! Set 30 minutes aside to sit down with your loved ones and talk about any diseases or disease risk factors, that are in your family. Awareness is the key to prevention!
Today is NAIRHHA Day! Every September 9th, the Hepatitis B Foundation brings awareness to National African Immigrant and Refugee HIV/AIDS and Hepatitis Awareness Day. Founded by advocates in Massachusetts, Washington D.C., and New York, NAIRHHA Day has been observed annually on September 9th by healthcare professionals, awareness campaigns, and other organizations since 2014. The Multicultural AIDS Coalition (MAC), Hepatitis B Foundation and the Coalition Against Hepatitis for People of African Origin (CHIPO) are working to establish NAIRHHA day as their own federally designated awareness day.
Hepatitis B and HIV in African Immigrant Communities
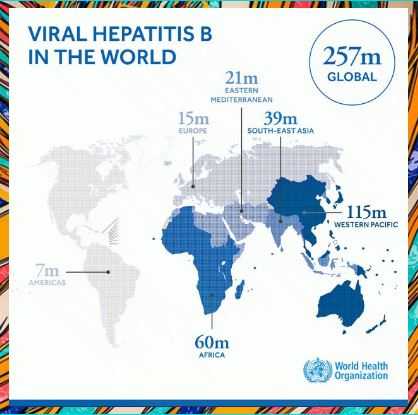
People of African origin are disproportionately affected by hepatitis B infection. Worldwide an estimated 292 million people are infected with chronic hepatitis B. Over 60 million people in Africa have hepatitis B which annually accounts for an estimated 68,870 deaths.1
In fact, in some African communities in the United States, between 5%-15% of people have chronic HBV infection. Unfortunately, due to the silent nature of the disease, lack of disease awareness, and limited health care access, most African community members who have hepatitis B DO NOT KNOW that they are infected. This puts them at much greater risk for premature death from cirrhosis or liver cancer.
There is a high burden of HIV/HBV co-infection in African countries because both diseases share similar transmission routes such as mother-to-child, unsafe medical and injection practices, and unscreened blood transfusions.2 Chronic HIV/HBV infection is reported in up to 36% of people who are HIV positive, with the highest prevalence reported in west Africa and southern Africa. The co-infection of HIV and HBV is especially dangerous because it accelerates liver disease such as fibrosis and cirrhosis. In fact, liver-related mortality is twice as high among people with an HIV/ HBV co-infection.2
With approximately 54,000 people with HBV who immigrate to the United States annually it is important to bring awareness to hepatitis B in African Immigrant communities on this day!
Get Involved
Viral hepatitis and HIV heavily impact African immigrant communities in the U.S. Let’s raise awareness and advocate for resources and funding to support elimination efforts & healthier communities.
Action Items:
There are African community organizations all over the U.S., from Boston to Seattle. Connect with one in your area to learn more about & contribute to the health of these vibrant communities. Start by visiting https://www.hepb.org/research-and-programs/chipo/member-organizations/
Data drives policy change & it can be difficult to find data about African immigrant communities because it is often not separated from data about African American communities. Advocate for this data to be separated by contacting your local Department of Health today!
Education & awareness matter! Many elected officials do not know about these issues, but they should! Contact your state & federal reps today to ask what they’re doing to address viral hepatitis & HIV in African immigrant communities. Visit https://www.usa.gov/elected-officials
Change needs resources! Help grow the capacity of African organizations in your area by contributing your time, money, or other resources to eliminating viral hepatitis & HIV in African immigrant communities. Find an org in your state or city & ask how you can plug into their work!
Funding is critical for progress to occur & advocacy is needed to make sure African immigrant communities receive enough money to combat viral hepatitis & HIV. Contact your federal, state, & local elected officials & local department of health to ask what they’re doing to support this. Start with members of @NASTAD found at https://www.nastad.org/membership-directory
Federal recognition means greater awareness, education, & resources. Continue to support the establishment of NAIRHHA Day as a federally recognized awareness day by contacting @HHS’s sitehiv.gov to advocate for this!
Spearman, C. W., Afihene, M., Ally, R., Apica, B., Awuku, Y., Cunha, L., Dusheiko, G., Gogela, N., Kassianides, C., Kew, M., Lam, P., Lesi, O., Lohouès-Kouacou, M. J., Mbaye, P. S., Musabeyezu, E., Musau, B., Ojo, O., Rwegasha, J., Scholz, B., Shewaye, A. B., … Gastroenterology and Hepatology Association of sub-Saharan Africa (GHASSA) (2017). Hepatitis B in sub-Saharan Africa: strategies to achieve the 2030 elimination targets. The lancet. Gastroenterology & hepatology, 2(12), 900–909. https://doi.org/10.1016/S2468-1253(17)30295-9
Are you a member of the African diaspora in the United States? Do you work for an organization that serves these communities? We would love for you to join CHIPO – the Coalition Against Hepatitis for People of African Origin! CHIPO is a national community coalition, co-founded and led by the Hepatitis B Foundation. Our members include a variety of individuals and organizations from all over the country, who are interested in and focused on addressing the high rates of hepatitis B among African communities in the US., which are disproportionately affected by hepatitis B and liver cancer. In some parts of the country, rates of chronic hepatitis B infection in African communities are estimated to range between 5 and 15% of people.
The purpose of CHIPO is to provide a space for an open exchange of ideas, best practices, and information about how to dismantle some of the many barriers that stand in the way of preventing, diagnosing, and treating chronic hepatitis B infection, and preventing liver cancer, in African immigrant communities. These barriers include a lack of disease awareness, high rates of stigma, limited access to healthcare and services, and the silent nature of the disease, which often does not present any symptoms until significant liver damage has occurred – a process which could take years or even decades. As a result, most African community members who have hepatitis B DO NOT KNOW that they are infected. This puts them at much greater risk for premature death from cirrhosis or liver cancer.
CHIPO, meaning “gift” in the Shona language, aims to disseminate accurate information about hepatitis B transmission, prevention, and treatment among community members, healthcare providers, and organizational leaders, and to improve the national capacity to raise hepatitis B awareness, testing, vaccination, and linkage to care among highly affected African communities. CHIPO also works to ensure that African immigrant communities are represented in HBV discussions and programs regionally and nationally. This is achieved through advocacy and the development of national and local partnerships. We currently have over 35 coalition partners around the U.S., dedicated to addressing viral hepatitis in African communities.
The activities of CHIPO are many and diverse. They include bimonthly virtual meetings, which often center around a presentation by a coalition member about measures or interventions that have been undertaken or research that has been done to achieve one of CHIPO’s objectives – namely improving awareness about and access to hepatitis B information, screening, vaccination, and linkage to follow-up care. Other activities include educational community events and presentations; supporting the design and implementation of initiatives to help accomplish CHIPO’s goals, such as the CDC Know Hepatitis B campaign (discussed below) and a recent grant from Bristol Myers Squibb to raise awareness about liver cancer and understanding about the link between hepatitis B and liver cancer in African immigrant communities; and promoting the work of coalition members locally and nationwide.
An example of a project for which CHIPO provided great support and guidance was the production of the first nationally available hepatitis B educational resources, specifically for African populations. Created in collaboration with the Centers for Disease Control and Prevention (CDC), these materials are part of a train-the-trainer-based model, and include a suite of materials, including a downloadable presentation on hepatitis B for community health workers, a printable flip chart for direct community education, and supporting fact sheets and resources. The presentation and flip chart have also been translated into Amharic, Arabic, French, and Swahili.
To read more about CHIPO, including previous blog posts, articles, and meeting minutes, and to access a full list of our members and the work they are doing around the country, visit our website.
Does this work sound interesting to you? Would you like to work with us to achieve lower rates of hepatitis B and liver cancer in African immigrant communities through increasing awareness, screening, vaccination, and linkage to care? Join us! Anyone is welcome to join CHIPO – contact the coordinator to get involved. We hope to see you on our next call!
On Monday September 21st, a virtual celebration was held in honor of the sixth anniversary of National African Immigrant and Refugee HIV and Hepatitis Awareness (NAIRHHA) Day. This day, which itself is commemorated on September 9th, was created to build awareness and dismantle stigma around HIV and viral hepatitis in African immigrant and refugee communities. It takes place in September because this is the month that has been designated as National African Immigrant Month (NAIM) in the United States to celebrate the diverse and remarkable contributions African immigrants have made to enrich the United States, in spheres ranging from sports to writing to politics.
The virtual celebration that occurred last Monday included a discussion of the history of NAIRHHA Day and how it came to exist in its present form, a conversation with a hepatitis B advocate who is living with the disease, discourse about the importance of NAIRHHA Day on the national level and implications for making it a federally recognized day, and trivia questions about HIV and hepatitis B.
History of NAIRHHA Day: The Journey from 2014 to Present
Moderator: Chioma Nnaji, MPH, MEd, Program Director, Multicultural AIDS Coalition
Panelists: Augustus Woyah, Program Officer for Minority AIDS Initiative, Maryland Department of Health
Amanda Lugg, Director of Advocacy and LGBTQ Programming, African Services Committee
The idea for NAIRHHA Day was first conceived in 2006 at a convening of the Ethiopian Community Development Corporation in Washington, DC, at a session sponsored by Office of Minority Health about HIV in African immigrant communities. Conferences started to occur, primarily in the Northeast, although there was also interest in Atlanta and Seattle. It seemed that an opportunity had finally become available for advocates, researchers, and providers to all come together and focus on data collection, community mobilization, and policy work around HIV and viral hepatitis in African immigrant communities. The African National HIV/AIDS Alliance was established in 2010 and awareness days started in 2012 (Augustus played a large role in this). In 2014, Chioma Nnaji became connected to Sylvie Bello, the Executive Director of the Cameroonian Association in Washington, DC, and they, along with Amanda and Augustus, worked to get NAIRHHA Day off the ground. Chioma has largely spearheaded efforts to have NAIRHHA Day recognized nationally.
In terms of some of the challenges that have and continue to exist around NAIRHHA Day, obtaining community leadership and organizational buy-in, as well as national attention, are at the forefront. Social media and other digital platforms have been widely used in order to amplify the cause and try to obtain federal recognition. Additionally, maintaining relationships with government agencies has been quite difficult and has become a clash of visions of sorts. There is a strong belief that NAIRHHA Day should be a community-driven effort, but government agencies often have their own priorities, which can be distinct from those of the community and grassroots organizers. This is not to discount the government and organizational partners that are still involved, however, including NASTAD, the Hepatitis B Foundation, CHIPO, CHIPO-NYC, and Africans for Improved Access at the Multicultural AIDS Coalition. Another challenge has been reinforcing the distinction between African immigrant and African American communities and not treating the Black community as a monolith. Drawing this distinction in both data and policy remains difficult, thus often rendering African immigrant communities invisible.
When pondering what areas could use improvement going forward, a number of different items were considered. These included incorporating COVID-19 into the conversation, along with viral hepatitis and HIV; addressing social and environmental determinants of health that lead to the over-prevalence of both infectious and non-communicable diseases in minority, and particularly African immigrant communities; adhering to the primary goal of community mobilization and including advocates and researchers to influence policy that provides linguistically and culturally appropriate services that address the most pressing issue of stigma; securing national attention; and obtaining resources. It is critical to remember that advocacy never ends, the need to magnify work and amplify voices is always present, there is no room for complacency, and there exists intersectionality in all issues (social and health justice are all-encompassing).
#justB Storyteller Interactive Discussion
Moderator: Farma Pene, Community Projects Coordinator in Viral Hepatitis Program, New York City Department of Health & Mental Hygiene
#justB Storyteller: Bright Ansah
In this session, Bright spoke about his experience with living with hepatitis B, including his diagnosis, treatment, and communication with his family. He spoke about being able to put a face to hepatitis B, which has helped many people and also allowed him to build strong relationships with a broader community. Bright found out about his status in 2014 and initially felt very lost. The first couple of years were a big struggle, as he did not want to worry his family and it took a while for him to come to peace with his diagnosis. This peace eventually came from a lot of extensive research, after which he found out that hepatitis B is not a death sentence and can be managed very well. He then started to think about what he could do to prevent someone else from becoming “a statistic.”
When asked what message he would share with newly diagnosed people, Bright stated that stress and anxiety are normal, but you are not alone. Every day, people find out they are infected. Bright has given his contact information to many different people and he emphasized the incredible importance of having a support system in place. When asked about how he overcame stigma and barriers, Bright replied that the biggest barrier is the mental hurdle. It took him about two years to not feel overwhelmed. Bright does still struggle with feeling rejected from clinical trials and finds this very frustrating – he still feels like he is being punished for having chronic hepatitis B.
The best advice that Bright can offer is to always be your own advocate and do your own research. If the first doctor or liver specialist that you find does not take you seriously or you feel that they are not doing enough for you, you do not need to stay with them and you can absolutely find another doctor. Bright went through this process himself and eventually found a doctor he likes at Johns Hopkins, through a friend of his. This can be a challenge with language barriers, but there are organizations that can help and there is a Specialist Directory tool on the Hepatitis B Foundation website, a resource that Bright stated he found very helpful, along with the website of the National Institutes of Health (NIH). Farma reiterated that the HBF website is a great place to visit to understand lab results in plain language, and offers a good collection of resources for family and community members of people living with hepatitis B. Bright finds that the most important questions to ask are: What exactly is your status and viral load? What should reasonable expectations for your life and health be? Is treatment appropriate and if so, which one? It is crucial to establish mutual respect with your doctor, and to iterate what expectations you have for your doctor as well. The most important messages are: Reach out. Ask questions. Stand up for yourself. You are not alone.
The Important Role that NAIRHHA Day Plays from a National and Policy Prospective
Moderator: Chioma Nnaji, MPH, MEd, Program Director, Multicultural AIDS Coalition
Panelists: Boatemaa Ntiri-Reid, JD, MPH, Hepatitis Director, NASTAD
Jennease Hyatt, Community Liaison for Boston/New England, GILEAD
The final conversation focused on why NAIRHHA Day should become a nationally recognized holiday. VIral hepatitis is the seventh leading cause of death globally. Nineteen million African adults are living with hep C, and 5-8% are living with hep B. Hep B and HIV need to be considered part of the health portfolio of African immigrants, with care taken that this does not compound stigma. NAIRHHA Day is really an opportunity to focus on this community specifically. You get things done by doing them yourselves and we are who we’ve been waiting for.
There is a strong need for a multi-faceted approach to this work and for local, state, and national partnerships. African immigrants need to be at the forefront of the HIV/AIDS conversation. In Massachusetts specifically, over half of new HIV infections are in immigrant communities: These communities need to be leading the conversation. In terms of the role that government agencies play in NAIRHHA day, this needs to be more than a supportive role. We need to talk about novel approaches. We know that there are healthcare disparities. We need to consider how to use funding to build capacity and engagement, and make sure this work moves forward. This should include counting in community members and small businesses and bringing people to the table who are not usually there. The community really wants to be engaged. Promoting testing and awareness at soccer games, for example, is a great idea. We need strong partnerships and leadership from the beginning and to determine different approaches and thus different outcomes. Community members are the experts and we need to treat them as such.
Across the country, there are jurisdictions that have a prevalence of 40,000 people living with hepatitis in a state and viral hepatitis staff have teams of 1-7. Local and state health departments have more of a role to play. CDC publishes a list of viral hepatitis coordinators by state. It would be great to close the gap with them and discuss more about what they are doing generally and how to get them more involved in NAIRHHA Day specifically. In thinking about a vision for NAIRHHA Day next year, thoughts included that everyone who serves African immigrant communities (including health centers and multi-service organizations) needs to see themselves as part of the solution. Additionally, federal representation should be part of NAIRHHA Day next year.
Trivia and Conclusion
The event concluded with trivia questions about HIV and hepatitis B prevention, testing, and treatment. Amazing music was provided by DJ WhySham and Laura O (@LauraO_TV) served as an excellent moderator. Thanks to everyone who participated and we look forward to another wonderful event next year!
National Family Health History Day is November 28th, and it is the perfect time to sit down and talk to your family about health; it gives your loved ones an opportunity to provide the gift of a healthy future! As hepatitis B rarely has any symptoms, many people do not discover that they are infected until a family member is diagnosed or they develop liver damage or liver cancer.
Approaching the topic and starting the conversation can help to break this cycle of transmission within families, and allow your loved ones to protect themselves. If you need some tips on how to start the discussion on family health, you can check out our blog post here!
Your family’s health history tells a powerful story. It guides us on what behaviors to avoid and actions that we can take to prevent developing certain illnesses or diseases. It can also help inform us on how to best navigate the health system. Do I need to be tested for liver cancer? Is the medication that I’m taking actually dangerous to my health?
When a family member is living with or has lived with hepatitis B, family health history can become even more critical to creating a healthy future. Hepatitis B is one of the world’s leading causes of liver cancer, so it is extremely important to be aware of your risk! Although hepatitis B is not genetic or hereditary – it is only spread through direct contact with infected blood or through sexual contact – multiple family members can be infected without knowing. This is because hepatitis B often does not have any symptoms and can be spread from mother to child during childbirth or by sharing sharp objects such as razors, toothbrushes, or body jewelry that may contain small amounts of infected blood. Knowing about a family members’ current or past infection is a signal to get tested for hepatitis B using the 3-panel hepatitis Bblood test (HBsAg, HBsAb, HBcAb). Testing is the only way to be sure of your hepatitis B status. The test will let you know if you have a current infection, have recovered for a past infection, or need to be vaccinated.
Why does this matter if myself or a family member has recovered from a past infection?
If someone has recovered from a past infection (either acute or chronic), this is great news! Loss of the hepatitis B surface antigen may be exciting, but it does not mean that you don’t need to proceed with caution! Recovery from a past infection means that while the virus is no longer in your blood, it is still living in the liver in an inactive state. You cannot infect anyone else at this stage, but family members, and sexual partners should still get tested for the 3-panel hepatitis B blood test (HBsAg, anti-HBc, anti-HBs) because they may have been exposed in the past. Check out this helpful fact sheet on what it means to have recovered from an acute or chronic infection!
A past infection should be a part of all medical records as well. Various medications and treatments for other conditions, such as cancer or Rheumatoid arthritis have the potential to reactivate the virus that is sleeping in your liver. Some medications can suppress the immune system, which gives hepatitis B a chance to reawaken and attack the liver. Healthcare providers need to be aware if you had a past infection so that they can monitor you and potentially prescribe medications to prevent the virus from reactivating in your body.
Not every treatment will cause hepatitis B to reactivate, so it is important to be aware of the ones that carry a risk! Any treatment that suppresses the immune system such as chemotherapy and other cancer therapies, and certain arthritis, Crohn’s disease, Ulcerative colitis, asthma, and psoriasis drugs may pose a risk of hepatitis B reactivation. You can find a list of specific drug names and their risk levels on our website, but you should always consult your doctor or provider for the most accurate information.
Every medication also comes with a warning label that you should read carefully. This section will let you know if there is a risk of reactivation. You can also use the National Institute of Health’s LiverTox website to search the name of treatment and see if there is a risk!
Talking to Your Family
Hepatitis B may increase a person’s risk of liver disease and liver cancer but with knowledge of an infection, you can take measures to help manage it. For family members who have not been infected, they can take action to prevent future infection by getting vaccinated! Many people assume that they have already been vaccinated, but this is not always the case. Globally, adult completion rates of all 3 doses of the vaccine are low, meaning that most adults are vulnerable to infection. The vaccine is highly effective and is the best form of protection against the virus. Don’t assume you have been vaccinated; check your immunization records or ask your doctor!
Spending your holiday talking about health may not sound like fun, but it is extremely important – it may even change your life! Set 30 minutes aside to sit down with your loved ones and talk about any diseases or disease risk factors, that are in your family. Awareness is the key to prevention!
Each year in September, the Hepatitis B Foundation recognizes National African Immigrant and Refugee HIV and Hepatitis Awareness Day (NAIRHHA). Founded by advocates in Massachusetts, Washington D.C., and New York, NAIRHHA Day has been observed annually on September 9th by healthcare professionals, awareness campaigns, and other organizations since 2014. Although not yet nationally recognized, the multicultural AIDS Coalition (MAC) and the Coalition Against Hepatitis B for People of African Origin (CHIPO) are working to establish NAIRHHA day as its own federally designated awareness day. As explained by Chioma Nnaji, Director at the Multicultural AIDS Coalition’s Africans For Improved Access (AFIA) program, there is a great need to establish NAIRHHA day as its own day. “Several of the current awareness days are inclusive of African immigrant communities, but do not comprehensively address their unique social factors, cultural diversity as well as divergent histories and experiences in the US.”
Why NAIRHHA Day?
People born outside of the U.S. often face different health challenges than those born in the country and face various barriers to accessing important healthcare services. African immigrants (AI) are disproportionately burdened by HIV and viral hepatitis. Advocates for NAIRHHA Day recognized the need to address these health issues in the community and thought that a combined awareness day would be the most effective way to reach the largest number of people impacted.
Hepatitis B presents a significant public health burden for many African countries, and subsequent immigrant populations living in the United States. Although data is limited on hepatitis B infection among African immigrant (AI) and refugee communities in the U.S., studies have shown infection rates are high – between 5 and 18%1,2,3,4,5. One community study in Minnesota even found AIs accounting for 30% of chronic hepatitis B infections 6. AI communities are also known to be disproportionately affected by HIV/AIDS, with diagnosis rates six times higher than the general U.S. population7. Despite this alarming disparity, HIV and hepatitis B awareness, prioritization, and funding has remained limited for this population.
Two of the largest barriers to testing for HIV and viral hepatitis among African immigrants are lack of awareness and stigma. Cultural and religious values shape the way people view illness, and there can be fears around testing and diagnosis of illness, and moral implications for why someone may feel they are at risk. While stigma about HIV/AIDS and hepatitis B often come from within one’s own community and culture, it is primarily driven by lack of awareness. Oftentimes, awareness is low in an individual’s home country because of limited hepatitis education, resources, and healthcare infrastructure. When they arrive in the U.S., awareness remains low for similar reasons. Community health workers and physicians are vital stakeholders to raise community awareness in a culturally sensitive way to help identify current infections and prevent future ones through vaccination.
Recognizing NAIRHHA Day is important in order to address the numerous barriers to prevention and treatment that African immigrants face. It was also founded to acknowledge the cultural and ethnic differences that influence how African-born individuals interact with their medical community and the concept of illness. The specific goals of the day of recognition include:
Raising awareness about HIV/AIDS and viral hepatitis to eliminate stigma;
Learning about ways to protect against HIV, viral hepatitis and other related diseases;
Taking control by encouraging screenings and treatment, including viral hepatitis vaccination;
Advocating for policies and practices that promote healthy African immigrant communities, families, and individuals.
What has been done so far?
The path to federal recognition has been a slow process, but progress has been made! Check out the timeline below for a brief overview of what has been accomplished since the day was created:
2014:
Inaugural city-wide events in Houston, Texas; Boston, Massachusetts; Washington D.C.; Maryland; Seattle, Washington; New York; Ohio and Philadelphia.
A national petitionwas created and 40% of the petitioners are from or live in Massachusetts; 60% of signers are from 33 other states across the US
2015:
Social Media efforts reached more than 500,000 individuals
Senator Elizabeth Warren gave a proclamation in Massachusetts
Created an informational blog post for the National Viral Hepatitis Roundtable
Joined the African immigrant Hepatitis/HIV Twitter chat (#AIHHchat)
2017:
Hosted a national webinar focused on barriers and strategies addressing HIV and hepatitis B among African immigrants
Official request to HIV.gov to officially recognize NAIRHHA Day
2018:
Hosted an online panel discussion addressing HIV and HBV stigma among African immigrant
New social media campaign
National Webinar with HBF and CHIPO focused on stigma
September marks the unofficial beginning of National AfricanImmigrant Heritage Month (NAIHM) – state and federal officials in over thirty states recognize September as NAIHM despite it not being federally declared – which is why NAIRHHA Day is held on September 9th. Federal recognition would significantly boost awareness within the community and allow for the creation of much-needed resources like culturally sensitive education tools. It would also help to disseminate the important health messages on a larger, national scale.
This year, the Hepatitis B Foundation and CHIPO are excited to be sponsoring four community events with partners throughout the U.S. to commemorate NAIRHHA day and promote hepatitis B and HIV education and testing in AI communities.
Contact Chioma, Director of the Multicultural AIDS Coalition, at cnnaji@mac-boston.org to get involved in advocacy for NAIRHHA Day
References:
Kowdley KV, Wang CC, Welch S, Roberts H, Brosgart CL. (2012). Prevalence of chronic hepatitis B among foreign-born persons living in the United States by country of origin. Hepatology, 56(2), 422-433. And Painter. 2011. The increasing burden of imported chronic hepatitis B—United States, 1974-2008. PLoS ONE 6(12): e27717.
Chandrasekar, E., Song, S., Johnson, M., Harris, A. M., Kaufman, G. I., Freedman, D., et al. (2016). A novel strategy to increase identification of African-born people with chronic hepatitis B virus infection in the Chicago metropolitan area, 2012-2014. Preventing Chronic Disease, 13, E118.
Edberg, M., Cleary, S., & Vyas, A. (2011). A trajectory model for understanding and assessing health disparities in Immigrant/Refugee communities. Journal of Immigrant and Minority Health, 13(3), 576-584.
Kowdley, K. V., Wang, C. C., Welch, S., Roberts, H., & Brosgart, C. L. (2012). Prevalence of chronic hepatitis B among foreign‐born persons living in the united states by country of origin. Hepatology, 56(2), 422-433.
Ugwu, C., Varkey, P., Bagniewski, S., & Lesnick, T. (2008). Sero-epidemiology of hepatitis B among new refugees to Minnesota. Journal of Immigrant and Minority Health, 10(5), 469-474.
Kim WR, Benson JT, Therneau TM, Torgerson HA, Yawn BP, Melton LJ 3d. Changing epidemiology of hepatitis B in a U.S. community. Hepatology 2004;39(3):811–6.
Blanas, D. A., Nichols, K., Bekele, M., Lugg, A., Kerani, R. P., & Horowitz, C. R. (2013). HIV/AIDS among African-born residents in the United States. Journal of immigrant and minority health, 15(4), 718–724.
We’re pleased to announce that the Hepatitis B Foundation (HBF) is now a member of NORD, the National Organization for Rare Disorders, representing our program, Hepatitis Delta Connect. NORD is a patient advocacy organization dedicated to individuals with rare diseases and the organizations that serve them. We will join 280 other patient organization members, all committed to the identification, treatment, and cure of rare disorders through programs of education, advocacy, research, and patient services.
Although globally, hepatitis delta is estimated to affect 15-20 million people, in the U.S. it is classified as a rare disease, as it is estimated to affect less than 200,000 people. The complicated nature of the virus and limited prioritization contribute to the gap in awareness, resources, testing practices and adequate treatments for hepatitis B and delta coinfection. Joining NORD will help amplify our voice, raise awareness about hepatitis delta in people living with chronic hepatitis B, provider and pharmaceutical communities and contribute to health policy efforts.
Hepatitis Delta Connect has previously been active with NORD through participating in rare disease Twitter chats and presenting a poster at the NORD Rare Action Summit in October 2018. We’re very excited to be a part of the coalition, and to be spreading awareness about hepatitis delta!
Meet Edwin Tan – a 29-year-old mechanical design engineer from Minneapolis, Minnesota! In 2014, Edwin was diagnosed with hepatitis B. Like many others living with hepatitis B, his diagnosis was a shock. Before his diagnosis, all he knew was that he was banned from giving blood to the Red Cross, but no one had explained the reason why. A routine blood test provided no explanations either, so his doctor decided to test for hepatitis B. The test revealed that Edwin was living with chronic hepatitis B.
After his diagnosis, Edwin decided to learn all that he could about the infection. Through his research, he found that one of the best ways to keep his liver healthy was through small lifestyle changes. Edwin began to pursue healthier life choices by increasing the amount of exercise he was getting and paying closer attention to his diet. Although he loved craft beer, he knew that drinking could be extremely dangerous to those with liver infections, so he willingly gave up all alcohol. Edwin’s dedication to a more active lifestyle led him to challenge himself by competing in local races and triathlons.
Edwin’s journey led him to realize that there is a lack of awareness about hepatitis B. He noticed that the stigmas facing those living with hepatitis B could take a physical and mental toll on an individual and impact how they viewed themselves. Edwin’s observations inspired him to reach out to the Hepatitis B Foundation to raise money and awareness for hepatitis B research, patient outreach, and education. Since his passion for racing was discovered due to his commitment to health after his diagnosis, it seemed appropriate for him to use his love of sports to fundraise for hepatitis B awareness and research! He hopes that his athletic achievements help others living with hepatitis B to realize that they are more than their infection.
Now, Edwin is training for a series of six races—triathlons, a marathon and an ironman – and we’ll be with him every step of the way! You can make a gift to support Edwin’s fundraising efforts here.
“I want to be a positive example against the stigma associated with Hep B and the shame that some people may feel for having it. Completing an Ironman, which is regarded as one of the most difficult one-day athletic events, serves as a good example that we each can accomplish anything we want as long as we believe in ourselves.”
To follow updates on Edwin’s journey, you can follow the Hepatitis BFoundation or Hep B United on Facebook. Be sure to use the hashtag #Tri4ACure!
North American Occupational Health and Safety Week (May 5-11) is a time to raise awareness about the importance of injury and illness prevention in the workplace! This week, we’re focusing on health and safety within the nail salon industry, specifically the risk for hepatitis B transmission and opportunities to increase awareness and education about hepatitis B among nail salon workers.
In the U.S., the nail salon workforce is comprised mostly of Vietnamese Americans, with many being immigrants. Refugee and immigrant communities are often susceptible to worker exploitation (including labor trafficking) and encounter cultural and linguistic barriers that may leave them vulnerable to occupational health and safety risks, including hepatitis B transmission.
During routine work, nail technicians may be exposed to a client’s blood or other bodily fluids. It is important for nail salon workers to take precautionary measures to protect themselves and their clients to prevent the potential spread of the hepatitis B virus. More importantly, the nail salon industry (including salon owners and state health departments or boards that regulate nail salons) should implement policies that support greater education, awareness, and prevention of hepatitis B transmission among its workforce.
In October of 2011, the American College of Gastroenterology urged the need for increased surveillance and information on disinfection and infectious disease prevention, particularly for hepatitis B and C in nail salons. Since then, no major research or analysis has been conducted to better understand hepatitis B transmission or the policies that protect nail salon workers. In a new report released by the Hepatitis B Foundation, “The Impact of Nail Salon Industry Policies and Regulations on Hepatitis B Awareness and Prevention,” we seek to further understand the nail salon industry landscape through analyzing state policies that govern nail salons and identify strategies to support increased hepatitis B education, awareness, and prevention.
The nail salon industry is regulated at the state level by a regulatory Board of Cosmetology that oversees and ensures nail technicians and nail salons comply with all rules and regulations. In this report, we analyze the nail salon workforce and industry regulations and provide recommendations that can address specific concerns. We conducted phone interviews with health clinics, public health workers, and other relevant stakeholders to better understand the challenges this population encounters when accessing hepatitis B education and care. In addition, we conducted a policy analysis of each state’s Board of Cosmetology to assess their effectiveness in protecting workers from exposure to bloodborne pathogens, specifically hepatitis B. In our analysis, we found that several states may not adequately protect workers from workplace hazards that may increase their risk of hepatitis B exposure. With sanitation and disinfection requirements that greatly vary between states, low compliance can leave workers susceptible to the transmission of bloodborne pathogens, including the hepatitis B virus.
We offered the following recommendations to provide industry changes and community initiatives that can help protect workers or link them to care:
Build partnerships between community organizations and nail salons to increase hepatitis B education, testing, and vaccination among nail salon workers
Integrate hepatitis B education into the nail technician licensing curriculum
Implement continuing education (CE) requirements around hepatitis B prevention and uphold sanitation requirements
Provide multilingual course training materials and written licensing exams
Adopt a sanitation rating system
Additionally, through our analysis, we found that four states have policies that discriminate against nail salon workers affected by hepatitis B by barring them from working in nail salons. Even with federal legal protections from the Americans with Disabilities Act, the continued discrimination in this industry presents a clear need to increase hepatitis B knowledge and awareness. Further state-level advocacy will be needed to address discriminatory policies. We must hold states accountable and advocate for policies and regulations that protect individuals affected by hepatitis B and prevent transmission of hepatitis B in the nail salon workplace.
Be sure to check out our full reportfor a detailed analysis of current state regulations and policies to assess their impact on educating and protecting nail salon workers and preventing hepatitis B transmission in the workplace.
Whether you work in a nail salon or visit one for a manicure or pedicure, be knowledgeable about the steps you can take to protect yourself. For further information about nail salon hazards and a complete guide to protecting your health and preventing injury in the workplace, check out OSHA’s guide here.





 discover that they are infected until a family member is diagnosed or they develop liver damage or liver cancer.
discover that they are infected until a family member is diagnosed or they develop liver damage or liver cancer. 
 HIV and viral hepatitis. Advocates for NAIRHHA Day recognized the need to address these health issues in the community and thought that a combined awareness day would be the most effective way to reach the largest number of people impacted.
HIV and viral hepatitis. Advocates for NAIRHHA Day recognized the need to address these health issues in the community and thought that a combined awareness day would be the most effective way to reach the largest number of people impacted. 
 NORD through participating in rare disease Twitter chats and presenting a poster at the NORD Rare Action Summit in October 2018. We’re very excited to be a part of the coalition, and to be spreading awareness about hepatitis delta!
NORD through participating in rare disease Twitter chats and presenting a poster at the NORD Rare Action Summit in October 2018. We’re very excited to be a part of the coalition, and to be spreading awareness about hepatitis delta!
 with hepatitis B could take a physical and mental toll on an individual and impact how they viewed themselves. Edwin’s observations inspired him to reach out to the Hepatitis B Foundation to
with hepatitis B could take a physical and mental toll on an individual and impact how they viewed themselves. Edwin’s observations inspired him to reach out to the Hepatitis B Foundation to
 The nail salon industry is regulated at the state level by a regulatory Board of Cosmetology that oversees and ensures nail technicians and nail salons comply with all rules and regulations. In this report, we analyze the nail salon workforce and industry regulations and provide recommendations that can address specific concerns. We conducted phone interviews with health clinics, public health workers, and other relevant stakeholders to better understand the challenges this population encounters when accessing hepatitis B education and care. In addition, we conducted a policy analysis of each state’s Board of Cosmetology to assess their effectiveness in protecting workers from exposure to bloodborne pathogens, specifically hepatitis B. In our analysis, we found that several states may not adequately protect workers from workplace hazards that may increase their risk of hepatitis B exposure. With sanitation and disinfection requirements that greatly vary between states, low compliance can leave workers susceptible to the transmission of bloodborne pathogens, including the hepatitis B virus.
The nail salon industry is regulated at the state level by a regulatory Board of Cosmetology that oversees and ensures nail technicians and nail salons comply with all rules and regulations. In this report, we analyze the nail salon workforce and industry regulations and provide recommendations that can address specific concerns. We conducted phone interviews with health clinics, public health workers, and other relevant stakeholders to better understand the challenges this population encounters when accessing hepatitis B education and care. In addition, we conducted a policy analysis of each state’s Board of Cosmetology to assess their effectiveness in protecting workers from exposure to bloodborne pathogens, specifically hepatitis B. In our analysis, we found that several states may not adequately protect workers from workplace hazards that may increase their risk of hepatitis B exposure. With sanitation and disinfection requirements that greatly vary between states, low compliance can leave workers susceptible to the transmission of bloodborne pathogens, including the hepatitis B virus.